Nutrients
Why vegetarian and vegan diets contain all the protein that you need

How Much Protein Do We Need?
Although protein is vital for our survival, we don’t need as much as is commonly believed. Recommended amounts have more than halved in the past 20 or so years as several chronic diseases have been linked to eating too much animal (not plant) protein. The average adult needs to consume between 45 and 55.5 grams of protein per day (COMA, 1991). We Westerners on average eat far more protein than we need. The maximum required, according to leading health bodies such as the World Health Organisation (WHO), is only around eight per cent of our energy (calories) from protein (Hegsted, 1968; Irwin and Hegsted,1975; Scrimshaw, 1976; COMA, 1991). Even this value includes a large safety margin, so most people’s real needs are even lower. Put simply, you practically have to be starving to be protein deficient, so it is ironic that we worry about this in our culture of plenty. Table 1 shows some of the current UK Reference Nutrient Intakes for protein. Values are given both in absolute terms (grams per day) and as a percentage of calories (the Estimated Average Requirement (EAR) for energy). To put these values into context internationally, rice provides around eight per cent of calories as protein and wheat around 17 per cent. The other major cereal staples lie between these two extremes. Only African millet is below this range (seven per cent). Some starchy roots, which are important staples, also fall below this range, such as cassava (three per cent), plantain (four per cent), sweet potato (four per cent) and yam (seven per cent) (Webb, 1995).
The Origins of the Protein Myth
The myth that we should eat more protein dates back to the beginning of the last century. The majority view back then was that health – and especially fitness – depended on eating generous amounts of protein, particularly meat (Millward, 2004). It was even reckoned that animal protein was the solution to wiping out child malnutrition in the third world (Autret, 1963; Gounelle de Pontanel, 1972; Stillings, 1973; Scrimshaw and Young, 1976). The myth reached epic heights in the 1960s. A UN report was published which identified worldwide protein deficiency. It called for a ‘global strategy to avert the impending protein crisis’. International aid began to focus on projects to address the so-called protein gap. The US government, for example, subsidised the production of dried milk powder to provide high-quality protein for the world’s poor (Campbell and Campbell, 2005). But not everyone accepted that protein was the most important nutrient of all. Wartime studies in the UK by Widdowson and McCance found that orphanage children grew faster than the general population when they ate a bread-based diet, with only a small fraction (14 per cent) of their protein coming from milk products. And the orphanage children grew no faster when nearly half of their protein was from milk! Bread provided the children with plenty of energy to support their growth, whilst meeting more than double their protein needs (Millward, 2004).
In truth, the protein gap disappeared ‘at the stroke of a pen’ in 1969 when researchers concluded that almost all staple foods contain enough protein for our needs.
Protein-energy Malnutrition
The main cause of death in children in developing countries is from something called protein-energy malnutrition. It usually develops in children who get too little protein and energy, and as the name of the condition reflects, these deficiencies tend to go hand-in-hand. Diets that contain enough energy (calories) typically contain plenty of protein, so the real problem is usually quantity, rather than quality of food. Grains supply the vast majority of the calories the world eats, and they provide protein too – even though most people equate protein with animal foods like meat, fish or dairy. In fact, all plant foods – grains, pulses (peas, beans and lentils), nuts, seeds and vegetables – contain protein. And most foods can easily provide us with the eight per cent of calories from protein recommended. The foods that are exceptions to this include fruits (which contain about five per cent of their energy from protein) and many sweets and junk foods. This makes it very easy to meet your protein needs and unnecessary to go out of your way to get protein in your diet.
• Protein dense foods – ie foods with a large number of grams
of protein per 100 grams of food – are more important for
adults, especially the elderly, than for infants or children.
• Energy dense foods – ie foods containing a large number of
calories per 100 grams of food – are more important for
children than for adults.
• Protein deficiency is more likely in the elderly than in children.
Although protein is vital for our survival, we don’t need as much as is commonly believed. Recommended amounts have more than halved in the past 20 or so years as several chronic diseases have been linked to eating too much animal (not plant) protein. The average adult needs to consume between 45 and 55.5 grams of protein per day (COMA, 1991). We Westerners on average eat far more protein than we need. The maximum required, according to leading health bodies such as the World Health Organisation (WHO), is only around eight per cent of our energy (calories) from protein (Hegsted, 1968; Irwin and Hegsted,1975; Scrimshaw, 1976; COMA, 1991). Even this value includes a large safety margin, so most people’s real needs are even lower. Put simply, you practically have to be starving to be protein deficient, so it is ironic that we worry about this in our culture of plenty. Table 1 shows some of the current UK Reference Nutrient Intakes for protein. Values are given both in absolute terms (grams per day) and as a percentage of calories (the Estimated Average Requirement (EAR) for energy). To put these values into context internationally, rice provides around eight per cent of calories as protein and wheat around 17 per cent. The other major cereal staples lie between these two extremes. Only African millet is below this range (seven per cent). Some starchy roots, which are important staples, also fall below this range, such as cassava (three per cent), plantain (four per cent), sweet potato (four per cent) and yam (seven per cent) (Webb, 1995).
The Origins of the Protein Myth
The myth that we should eat more protein dates back to the beginning of the last century. The majority view back then was that health – and especially fitness – depended on eating generous amounts of protein, particularly meat (Millward, 2004). It was even reckoned that animal protein was the solution to wiping out child malnutrition in the third world (Autret, 1963; Gounelle de Pontanel, 1972; Stillings, 1973; Scrimshaw and Young, 1976). The myth reached epic heights in the 1960s. A UN report was published which identified worldwide protein deficiency. It called for a ‘global strategy to avert the impending protein crisis’. International aid began to focus on projects to address the so-called protein gap. The US government, for example, subsidised the production of dried milk powder to provide high-quality protein for the world’s poor (Campbell and Campbell, 2005). But not everyone accepted that protein was the most important nutrient of all. Wartime studies in the UK by Widdowson and McCance found that orphanage children grew faster than the general population when they ate a bread-based diet, with only a small fraction (14 per cent) of their protein coming from milk products. And the orphanage children grew no faster when nearly half of their protein was from milk! Bread provided the children with plenty of energy to support their growth, whilst meeting more than double their protein needs (Millward, 2004).
In truth, the protein gap disappeared ‘at the stroke of a pen’ in 1969 when researchers concluded that almost all staple foods contain enough protein for our needs.
Protein-energy Malnutrition
The main cause of death in children in developing countries is from something called protein-energy malnutrition. It usually develops in children who get too little protein and energy, and as the name of the condition reflects, these deficiencies tend to go hand-in-hand. Diets that contain enough energy (calories) typically contain plenty of protein, so the real problem is usually quantity, rather than quality of food. Grains supply the vast majority of the calories the world eats, and they provide protein too – even though most people equate protein with animal foods like meat, fish or dairy. In fact, all plant foods – grains, pulses (peas, beans and lentils), nuts, seeds and vegetables – contain protein. And most foods can easily provide us with the eight per cent of calories from protein recommended. The foods that are exceptions to this include fruits (which contain about five per cent of their energy from protein) and many sweets and junk foods. This makes it very easy to meet your protein needs and unnecessary to go out of your way to get protein in your diet.
• Protein dense foods – ie foods with a large number of grams
of protein per 100 grams of food – are more important for
adults, especially the elderly, than for infants or children.
• Energy dense foods – ie foods containing a large number of
calories per 100 grams of food – are more important for
children than for adults.
• Protein deficiency is more likely in the elderly than in children.
What about Protein Quality?
To make protein, plants combine sugars (which they make from sunlight, carbon dioxide and water) with nitrogen from the air or soil. The end products are protein building blocks called amino acids. There are 20 or so different amino acids in your body, of which your body can make about 11 just from carbohydrate, fat and nitrogen (from protein) in your diet. Nine of the amino acids are called ‘essential amino acids’ which must be supplied by your diet as your body can’t make them (Geissler and Powers, 2005). Animal and soya products are called complete proteins as they contain plenty of all of the essential amino acids. However, most plant proteins lack one or more of the essential amino acids. There is a persistent myth that vegetarians need to be well,educated and choose protein foods that make up for the amino acid deficiencies of each other. But research shows that this is unnecessary and that both vegetarians and omnivores get enough protein, including plenty of the amino acids they need, as long as they are getting enough calories. People can obtain all of the essential amino acids they need from the natural variety of plant proteins eaten each day (Campbell and Campbell, 2005). Especially good sources of high quality protein include soya products (tofu, soya milk, veggie mince), cereals (rice, pasta, wholemeal bread), pulses (baked beans, chickpeas, kidney beans, lentils), nuts and seeds (pumpkin, sesame). To give you a comparison between some meat and vegetarian products, a standard 50g beef burger contains 10.2g of protein and three (90g) fish sticks 12.l g; half a 225g can of baked beans contains 11.5g of protein; an average serving of pasta (190g cooked) contains 8.5g, an average serving of kidney beans (160g cooked) 12.4g, and a small packet (25g) of peanuts contains 6.1g.
Why Do We Need Protein?
Proteins play an important role in the body, forming the basis of your muscles, hair, nails and collagen (the connective tissue that holds your body together). They are also required for the synthesis of various metabolic products, including neurotransmitters, thyroid hormones, haem (found in red blood cells), and nucleic acids (DNA and RNA). DNA and RNA determine the inherited characteristics of every living thing and play an important role in protein synthesis. It goes without saying that protein deficiency can wreak havoc on the body. But it can’t be stressed too often that protein deficiency usually goes hand-in-hand with energy deficiency, so don’t worry about it.
To make protein, plants combine sugars (which they make from sunlight, carbon dioxide and water) with nitrogen from the air or soil. The end products are protein building blocks called amino acids. There are 20 or so different amino acids in your body, of which your body can make about 11 just from carbohydrate, fat and nitrogen (from protein) in your diet. Nine of the amino acids are called ‘essential amino acids’ which must be supplied by your diet as your body can’t make them (Geissler and Powers, 2005). Animal and soya products are called complete proteins as they contain plenty of all of the essential amino acids. However, most plant proteins lack one or more of the essential amino acids. There is a persistent myth that vegetarians need to be well,educated and choose protein foods that make up for the amino acid deficiencies of each other. But research shows that this is unnecessary and that both vegetarians and omnivores get enough protein, including plenty of the amino acids they need, as long as they are getting enough calories. People can obtain all of the essential amino acids they need from the natural variety of plant proteins eaten each day (Campbell and Campbell, 2005). Especially good sources of high quality protein include soya products (tofu, soya milk, veggie mince), cereals (rice, pasta, wholemeal bread), pulses (baked beans, chickpeas, kidney beans, lentils), nuts and seeds (pumpkin, sesame). To give you a comparison between some meat and vegetarian products, a standard 50g beef burger contains 10.2g of protein and three (90g) fish sticks 12.l g; half a 225g can of baked beans contains 11.5g of protein; an average serving of pasta (190g cooked) contains 8.5g, an average serving of kidney beans (160g cooked) 12.4g, and a small packet (25g) of peanuts contains 6.1g.
Why Do We Need Protein?
Proteins play an important role in the body, forming the basis of your muscles, hair, nails and collagen (the connective tissue that holds your body together). They are also required for the synthesis of various metabolic products, including neurotransmitters, thyroid hormones, haem (found in red blood cells), and nucleic acids (DNA and RNA). DNA and RNA determine the inherited characteristics of every living thing and play an important role in protein synthesis. It goes without saying that protein deficiency can wreak havoc on the body. But it can’t be stressed too often that protein deficiency usually goes hand-in-hand with energy deficiency, so don’t worry about it.
Too Much of a Good Thing?
Excess animal protein on the other hand, is linked with kidney disease, osteoporosis, cancers, type 2 diabetes and cardiovascular disease – and usually results from eating too many animal products. Animal products, even lean-looking meats, are often associated with large amounts of saturated fat and cholesterol – artery clogging substances which are a main cause of heart disease, kidney failure and stroke as well as many cancers. But putting these hidden nasties aside, there is strong evidence to suggest it is excess protein per se which plays a part in all of these diseases. There is a compelling case that animal proteins – independent of other associated nutrients – increase the risk for cancer, atherosclerosis, osteoporosis and type 2 diabetes (Yang et al., 2002; Holmes et al., 2003; Sieri et al., 2002; O’Keefe et al., 1999; Campbell et al., 1998; Campbell and Junshi, 1994; Messina and Messina, 2000; Hu et al., 1993; Song et al., 2004). This was particularly evident in the China Study – one of the largest and most comprehensive studies ever undertaken to examine the relationship between diet and disease. Huge differences were seen in disease rates based on the amount of plant foods participants ate compared to animal foods (Campbell et al., 1993; Campbell and Junshi, 1994; Campbell and Campbell, 2005). Age-old Questions, Modern Day Solutions Though boosting protein supply could improve nutrition in the third world, it’s not the only way and neither is it the best for long-term health. Countries whose people are starving are using their land to grow grain for export to feed the West’s farmed animals. Nutritionally valuable food is being fed to animals to produce meat, but by not using animals as meat producing machines, this food could be freed to help those that need it most. Vegetarian (and more so, vegan) diets use up far less of the world’s resources of food, land water and energy, and are a positive step we can all easily take to help feed people in poorer countries. By eating a range of whole, plant-based foods you will get all the different amino acids you need – and in the right proportions. There is no need to go out of your way to get protein or specific amino acids or amino acid combinations. Rest assured that plant proteins can do a better job of meeting your protein needs than animal products, both because they are less concentrated sources of protein (making it less likely that you’ll get too much) and because they are more likely to be present with other nutrients such as fibre, vitamins, minerals, phytochemicals and healthy fats.
Excess animal protein on the other hand, is linked with kidney disease, osteoporosis, cancers, type 2 diabetes and cardiovascular disease – and usually results from eating too many animal products. Animal products, even lean-looking meats, are often associated with large amounts of saturated fat and cholesterol – artery clogging substances which are a main cause of heart disease, kidney failure and stroke as well as many cancers. But putting these hidden nasties aside, there is strong evidence to suggest it is excess protein per se which plays a part in all of these diseases. There is a compelling case that animal proteins – independent of other associated nutrients – increase the risk for cancer, atherosclerosis, osteoporosis and type 2 diabetes (Yang et al., 2002; Holmes et al., 2003; Sieri et al., 2002; O’Keefe et al., 1999; Campbell et al., 1998; Campbell and Junshi, 1994; Messina and Messina, 2000; Hu et al., 1993; Song et al., 2004). This was particularly evident in the China Study – one of the largest and most comprehensive studies ever undertaken to examine the relationship between diet and disease. Huge differences were seen in disease rates based on the amount of plant foods participants ate compared to animal foods (Campbell et al., 1993; Campbell and Junshi, 1994; Campbell and Campbell, 2005). Age-old Questions, Modern Day Solutions Though boosting protein supply could improve nutrition in the third world, it’s not the only way and neither is it the best for long-term health. Countries whose people are starving are using their land to grow grain for export to feed the West’s farmed animals. Nutritionally valuable food is being fed to animals to produce meat, but by not using animals as meat producing machines, this food could be freed to help those that need it most. Vegetarian (and more so, vegan) diets use up far less of the world’s resources of food, land water and energy, and are a positive step we can all easily take to help feed people in poorer countries. By eating a range of whole, plant-based foods you will get all the different amino acids you need – and in the right proportions. There is no need to go out of your way to get protein or specific amino acids or amino acid combinations. Rest assured that plant proteins can do a better job of meeting your protein needs than animal products, both because they are less concentrated sources of protein (making it less likely that you’ll get too much) and because they are more likely to be present with other nutrients such as fibre, vitamins, minerals, phytochemicals and healthy fats.
|
Summary
• Proteins form the basis of muscles, hair, nails and collagen. They are also needed to make a variety of other molecules, including neurotransmitters, thyroid hormones, haem, DNA and RNA. • Diets that contain enough energy (calories) typically contain plenty of protein. Most foods can easily provide us with the eight per cent calories from protein which the World Health Organisation recommends. • Western vegetarians and vegans get enough protein, including plenty of the amino acids they need, as long as they are getting enough energy (calories). |
• Especially good sources of high quality protein include soya
products, cereals, pulses, nuts and seeds. • The average adult needs to consume between 45 and 55.5 grams of protein per day. • Excess animal protein is linked with kidney disease, osteoporosis, cancers, type 2 diabetes and cardiovascular disease. • Plant proteins can do a better job of meeting your protein needs than animal products, both because they are less concentrated sources of protein (making it less likely that you’ll get too much) and because they are more likely to be present with other nutrients such as fibre, vitamins, minerals, phytochemicals and healthy fats. |
How a plant-based diet provides all the essential fats you need – and why animal fats are particularly detrimental to health

What is Fat and Why Do We Need It?
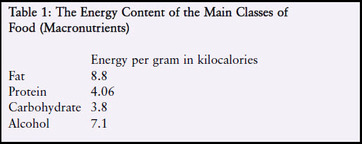
Of the four main classes of food, fat is the most energy dense. It contains more than twice as many calories (kilocalories) weight for- weight as protein or carbohydrate (see Table 1). It is a good source of energy, both for immediate use and for laying down a storage depot (adipose tissue) for use when food intake is reduced.
Fat in the diet helps the body to absorb fat-soluble vitamins (A, D, E and K). It is a source of the essential fatty acids that the body cannot make itself. Fat also provides insulation, protects the body’s vital organs and acts as a shock absorber. Fat’s more technical name is ‘lipid’ – a term that includes both fats and oils. Nominally, fats are solid at room temperature, oils are liquid, and dense brittle fats are called waxes. Lipids in the diet can come from both plants and animals. Plants most often store their oils in seeds, such as nuts, sunflower seeds, soya beans and corn; and sometimes in fruits, eg avocados, olives and coconuts. Animals most commonly store fat within their muscles (commonly called marbling fat), between their muscles, under their skin and around their gut area. Lipids in the diet are largely made up of molecules called fatty acids, attached to the molecule glycerol. Three fatty acids combine with one molecule of glycerol to form ‘triglycerides’. The fatty acids can be of three major types – saturated, monounsaturated and polyunsaturated, depending on how many double bonds they contain. A certain type of unsaturated fatty acid – trans unsaturated, or trans fatty acids’ – is often considered separately because of its ill effects on health, and because it is largely created by the
manufacturing process. The human body cannot function without some fat, but it is eating the right kind of fat that is vital in terms of our overall health. According to the Committee on Medical Aspects of Food Policy, most people should aim to get no more than 10 per cent (and preferably less than seven per cent) of their total calorie intake from saturated fat. Less than 10 per cent of calories should come from polyunsaturated fat. The 10 per cent figure for polyunsaturates includes one to two per cent of calories from omega-3 fats (Department of Health, 1991). Less than one per cent of calories – and preferably none – should come from trans fatty acids.
manufacturing process. The human body cannot function without some fat, but it is eating the right kind of fat that is vital in terms of our overall health. According to the Committee on Medical Aspects of Food Policy, most people should aim to get no more than 10 per cent (and preferably less than seven per cent) of their total calorie intake from saturated fat. Less than 10 per cent of calories should come from polyunsaturated fat. The 10 per cent figure for polyunsaturates includes one to two per cent of calories from omega-3 fats (Department of Health, 1991). Less than one per cent of calories – and preferably none – should come from trans fatty acids.
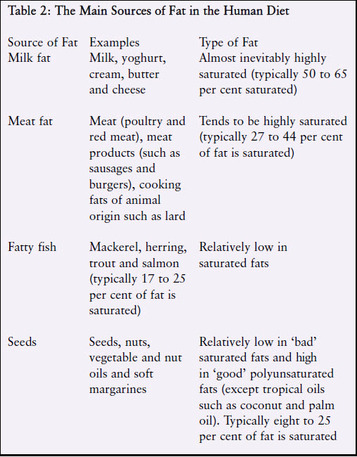
Table 2 summarises the main sources of fat in the human diet. Any food that contains any of these products as an ingredient will also contain fat.
Dietary Cholesterol Cholesterol is a soft, waxy substance found in the bloodstream and in all the body's cells. It is used to form cell membranes and some hormones. However, a high level of cholesterol in the blood (hypercholesterolaemia) is a major risk factor for heart disease. Cholesterol and other fats have to be transported to and from the cells by special carriers called lipoproteins. Two of particular note are low-density lipoprotein (LDL) and high-density lipoprotein (HDL). LDL is the major cholesterol carrier in the blood. Too much LDL cholesterol in the blood can lead to the build up of fatty deposits (plaques) on the inside walls of the arteries. Plaques can clog the arteries feeding the heart and brain (atherosclerosis); hence LDL is termed ‘bad’ cholesterol. Lower levels of LDL cholesterol reflect a lower risk of heart disease. HDL, on the other hand, tends to carry cholesterol away from the arteries and back to the liver, where it is eliminated from the body. A high HDL level seems to protect against heart disease, hence HDL cholesterol is termed ‘good’ cholesterol. Cholesterol comes from two main sources. The body produces approximately 1,000 milligrams per day. Animal products also contain cholesterol, especially egg yolks, meat, poultry, shellfish and whole- and reduced-fat milk and dairy. One small grilled skinless chicken breast contains 94 milligrams of cholesterol (FSA, 2002), whereas foods from all plants (every type of fruit and vegetable, pulses, (peas, beans and lentils) wholegrains, nuts and seeds) are cholesterol-free. Humans have no need for dietary cholesterol as the body can manufacture all that it requires. The American Heart Association recommends that people limit their average daily cholesterol intake to no more than 300 milligrams (AHA, 2008). High intakes of dietary cholesterol increase harmful LDL cholesterol (Grundy and Denke, 1990) which can increase the risk of heart disease. If you are genetically prone to hypercholesterolaemia then it is especially important to restrict dietary cholesterol, which is found in all animal products. Highquality proteins from vegetable sources such as pulses are good substitutes for animal sources of protein. For more information, see the VVF guide, Have a Heart.
Saturated Fatty Acids
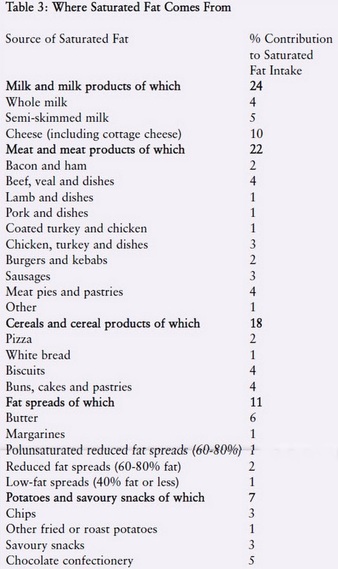
We have no nutritional need for saturated and monounsaturated fats as the body can make them. Diets high in saturated fat and calories raise blood cholesterol levels and contribute to cardiovascular disease, diabetes and some cancers. Saturated fat has 10 times the cholesterol-raising power of dietary cholesterol (Enas et al., 2003). Furthermore, foods high in saturated fat generally contain substantial amounts of dietary cholesterol. Reducing total and saturated fat intakes could also lower the risk of breast cancer (see VVF report, One in Nine). Table 3 illustrates the major sources of saturated fats in the UK national diet. Not all saturated fatty acids have the same effects. Those which raise cholesterol the most are lauric acid, myristic acid, and palmitic acid, which are found in meat, dairy products, eggs and tropical oils. These three fatty acids account for 60 to 70 per cent of the saturated fat in Western diets. Myristic acid is the most powerful cholesterol-raising saturated fatty acid (Kris-Etherton et al., 1997). The major dietary sources of myristic acid are butter, cream, whole milk and tropical oils. Milk fat (from dairy cows) contains eight to 14 per cent myristic acid. Coconut and palm oils contain up to 18 per cent (German et al., 2004). Palmitic acid is the most common fatty acid in the human diet. It is the main saturated fatty acid in animal fats (including red meats, poultry and eggs) and in palm oil. Lauric acid is the least harmful of these three saturated fats, with around one-third less cholesterol-raising power than palmitic acid. It is the main saturated fatty acid in coconut and palm kernel oils (they contain around 48 per cent) (Grundy, 1986; Renaud and Delorgel, 1989; Katan et al., 1995). As tropical oils such as coconut and palm do not feature heavily in our typical national diet, they do not contribute significantly to average national saturated fat intake (FSA/Department of Health, 2003). However, coconut is the main source of energy for certain Polynesian populations. The habitual diets of the toll dwellers from both Pukapuka and Tokelau are high in saturated fat (primarily from coconut) but low in dietary cholesterol (found only in animal products) and sucrose (sugar). Tokelauans take in many more calories from coconut than the Pukapukans (63 per cent compared with 34 per cent) and therefore have higher intakes of saturated fat. As might be expected, Tokelauans have higher blood cholesterol levels.
Dietary Cholesterol Cholesterol is a soft, waxy substance found in the bloodstream and in all the body's cells. It is used to form cell membranes and some hormones. However, a high level of cholesterol in the blood (hypercholesterolaemia) is a major risk factor for heart disease. Cholesterol and other fats have to be transported to and from the cells by special carriers called lipoproteins. Two of particular note are low-density lipoprotein (LDL) and high-density lipoprotein (HDL). LDL is the major cholesterol carrier in the blood. Too much LDL cholesterol in the blood can lead to the build up of fatty deposits (plaques) on the inside walls of the arteries. Plaques can clog the arteries feeding the heart and brain (atherosclerosis); hence LDL is termed ‘bad’ cholesterol. Lower levels of LDL cholesterol reflect a lower risk of heart disease. HDL, on the other hand, tends to carry cholesterol away from the arteries and back to the liver, where it is eliminated from the body. A high HDL level seems to protect against heart disease, hence HDL cholesterol is termed ‘good’ cholesterol. Cholesterol comes from two main sources. The body produces approximately 1,000 milligrams per day. Animal products also contain cholesterol, especially egg yolks, meat, poultry, shellfish and whole- and reduced-fat milk and dairy. One small grilled skinless chicken breast contains 94 milligrams of cholesterol (FSA, 2002), whereas foods from all plants (every type of fruit and vegetable, pulses, (peas, beans and lentils) wholegrains, nuts and seeds) are cholesterol-free. Humans have no need for dietary cholesterol as the body can manufacture all that it requires. The American Heart Association recommends that people limit their average daily cholesterol intake to no more than 300 milligrams (AHA, 2008). High intakes of dietary cholesterol increase harmful LDL cholesterol (Grundy and Denke, 1990) which can increase the risk of heart disease. If you are genetically prone to hypercholesterolaemia then it is especially important to restrict dietary cholesterol, which is found in all animal products. Highquality proteins from vegetable sources such as pulses are good substitutes for animal sources of protein. For more information, see the VVF guide, Have a Heart.
Saturated Fatty Acids
We have no nutritional need for saturated and monounsaturated fats as the body can make them. Diets high in saturated fat and calories raise blood cholesterol levels and contribute to cardiovascular disease, diabetes and some cancers. Saturated fat has 10 times the cholesterol-raising power of dietary cholesterol (Enas et al., 2003). Furthermore, foods high in saturated fat generally contain substantial amounts of dietary cholesterol. Reducing total and saturated fat intakes could also lower the risk of breast cancer (see VVF report, One in Nine). Table 3 illustrates the major sources of saturated fats in the UK national diet. Not all saturated fatty acids have the same effects. Those which raise cholesterol the most are lauric acid, myristic acid, and palmitic acid, which are found in meat, dairy products, eggs and tropical oils. These three fatty acids account for 60 to 70 per cent of the saturated fat in Western diets. Myristic acid is the most powerful cholesterol-raising saturated fatty acid (Kris-Etherton et al., 1997). The major dietary sources of myristic acid are butter, cream, whole milk and tropical oils. Milk fat (from dairy cows) contains eight to 14 per cent myristic acid. Coconut and palm oils contain up to 18 per cent (German et al., 2004). Palmitic acid is the most common fatty acid in the human diet. It is the main saturated fatty acid in animal fats (including red meats, poultry and eggs) and in palm oil. Lauric acid is the least harmful of these three saturated fats, with around one-third less cholesterol-raising power than palmitic acid. It is the main saturated fatty acid in coconut and palm kernel oils (they contain around 48 per cent) (Grundy, 1986; Renaud and Delorgel, 1989; Katan et al., 1995). As tropical oils such as coconut and palm do not feature heavily in our typical national diet, they do not contribute significantly to average national saturated fat intake (FSA/Department of Health, 2003). However, coconut is the main source of energy for certain Polynesian populations. The habitual diets of the toll dwellers from both Pukapuka and Tokelau are high in saturated fat (primarily from coconut) but low in dietary cholesterol (found only in animal products) and sucrose (sugar). Tokelauans take in many more calories from coconut than the Pukapukans (63 per cent compared with 34 per cent) and therefore have higher intakes of saturated fat. As might be expected, Tokelauans have higher blood cholesterol levels.
However, cardiovascular disease – the build up of lipids and other cells on the artery wall – is still surprisingly rare in both populations (Prior et al., 1981). This apparent paradox might be explained by coconut’s fibre content. Coconut is a good source of soluble and insoluble dietary fibre which have cholesterol-lowering powers. Coconut flakes (rather than coconut oil) have been found to lower harmful (LDL) cholesterol levels (Trinidad et al., 2004). Of course, processing coconut in order to produce coconut oil does strip away the protective fibre. Conversely, the leading sources of harmful saturated fats in the British national diet – namely dairy products and meat – contain no protective, cholesterol-lowering fibre (FSA, 2002; FSA/Department of Health, 2003). As perhaps would be expected, cardiovascular disease is a common finding in people who consume the modern Western diet. For more information, see VVF fact sheet, Plant-based Diets and Cardiovascular Disease.
Trans-unsaturated Fatty Acids
Trans fatty acids have also been shown to increase the risk of heart disease by raising harmful (LDL) cholesterol levels and lowering protective (HDL) cholesterol levels. Their combined effect on LDL and HDL cholesterol is twice that of saturated fatty acids (Mensink and Katan, 1990). Gram for gram, trans fats are even more strongly linked to heart disease than saturated fats. A review of trans fats’ effects on health found them to be associated with a two-and-a-half to tenfold higher risk of heart disease than saturated fats (Stender and Dyerberg, 2004). No safe limits of trans fat consumption have been identified (Murray, 2005). Trans fatty acids are often found in processed foods. An industrial process known as hydrogenation is often used to convert liquid vegetable oils to solid or semi-solid fats, such as those present in margarine. The final product of this process is called hydrogenated vegetable oil, or hydrogenated fat. It is used in some biscuits, cakes, pastry, margarine and many processed foods. Foods that contain hydrogenated vegetable oil (which is always declared in the ingredients list) are likely to contain trans fats. By avoiding products containing hydrogenated fats or oils the trans fat content of a plant-based diet can be kept desirably low. Low levels of trans fatty acids are also found naturally in dairy products, lamb and beef fat. This is because small amounts of trans fats are produced in the gastrointestinal tract of ruminant animals (Murray, 2005).
Trans-unsaturated Fatty Acids
Trans fatty acids have also been shown to increase the risk of heart disease by raising harmful (LDL) cholesterol levels and lowering protective (HDL) cholesterol levels. Their combined effect on LDL and HDL cholesterol is twice that of saturated fatty acids (Mensink and Katan, 1990). Gram for gram, trans fats are even more strongly linked to heart disease than saturated fats. A review of trans fats’ effects on health found them to be associated with a two-and-a-half to tenfold higher risk of heart disease than saturated fats (Stender and Dyerberg, 2004). No safe limits of trans fat consumption have been identified (Murray, 2005). Trans fatty acids are often found in processed foods. An industrial process known as hydrogenation is often used to convert liquid vegetable oils to solid or semi-solid fats, such as those present in margarine. The final product of this process is called hydrogenated vegetable oil, or hydrogenated fat. It is used in some biscuits, cakes, pastry, margarine and many processed foods. Foods that contain hydrogenated vegetable oil (which is always declared in the ingredients list) are likely to contain trans fats. By avoiding products containing hydrogenated fats or oils the trans fat content of a plant-based diet can be kept desirably low. Low levels of trans fatty acids are also found naturally in dairy products, lamb and beef fat. This is because small amounts of trans fats are produced in the gastrointestinal tract of ruminant animals (Murray, 2005).
Essential Fatty Acids
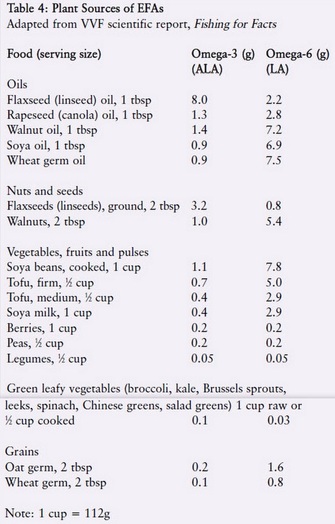
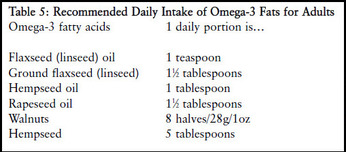
The fats which are essential to the diet are linoleic acid (from the omega-6 family of fatty acids) and alpha-linolenic acid (omega-3 family). Dietary sources of these essential fatty acids, or EFAs, are listed in Table 4. Seed oils such as flax (linseed), rapeseed (canola) and walnut oil are rich sources of EFAs as are seeds and nuts themselves (Buttriss, 1999). Green leafy vegetables are also a source (Pereira et al., 2001). Polyunsaturated fatty acids have many important functions in the body. They have a structural function in cell membranes; can aid the retina and other organs, including the brain and skin; are involved in regulating the transport, breakdown and excretion of cholesterol; and are precursors of prostaglandins, thromboxane and leukotrienes, which regulate many body processes including inflammation and blood clotting. There are at least three important fatty acids in the omega-3 family: ALA, EPA and DHA. ALA can be obtained from flaxseed (linseed) oil, walnuts, rapeseed, soya beans and green leafy vegetables (although the latter do not contain much as they are generally very low in fat) (see Table 4). EPA and DHA – which are required for brain function – can only be obtained from marine sources, namely oily fish and some species of algae. However, ALA can be converted into EPA and DHA in the body. Likewise, LA, found in sunflower, corn, walnut and soya oils, can be converted into other important polyunsaturated fatty acids in the omega-6 family, such as arachidonic acid.
The fats which are essential to the diet are linoleic acid (from the omega-6 family of fatty acids) and alpha-linolenic acid (omega-3 family). Dietary sources of these essential fatty acids, or EFAs, are listed in Table 4. Seed oils such as flax (linseed), rapeseed (canola) and walnut oil are rich sources of EFAs as are seeds and nuts themselves (Buttriss, 1999). Green leafy vegetables are also a source (Pereira et al., 2001). Polyunsaturated fatty acids have many important functions in the body. They have a structural function in cell membranes; can aid the retina and other organs, including the brain and skin; are involved in regulating the transport, breakdown and excretion of cholesterol; and are precursors of prostaglandins, thromboxane and leukotrienes, which regulate many body processes including inflammation and blood clotting. There are at least three important fatty acids in the omega-3 family: ALA, EPA and DHA. ALA can be obtained from flaxseed (linseed) oil, walnuts, rapeseed, soya beans and green leafy vegetables (although the latter do not contain much as they are generally very low in fat) (see Table 4). EPA and DHA – which are required for brain function – can only be obtained from marine sources, namely oily fish and some species of algae. However, ALA can be converted into EPA and DHA in the body. Likewise, LA, found in sunflower, corn, walnut and soya oils, can be converted into other important polyunsaturated fatty acids in the omega-6 family, such as arachidonic acid.
Why Plant Iron is Best

One of the commonest food myths is that vegetarians and vegans have a higher risk of iron deficiency
anaemia because they don’t eat meat. This is simply not the case and many major health organisations
agree – the British Medical Association, the World Health Organisation and the American Dietetic Association. However, some so-called ‘health’ organisations, health professionals and food writers persist in promoting red meat as the best source of iron. They invariably fail to mention the health risks
associated with the type of iron found in meat as opposed to iron from plants. This fact sheet debunks the Western myth of promoting meat as a good source of iron and explains why plant iron is best.
anaemia because they don’t eat meat. This is simply not the case and many major health organisations
agree – the British Medical Association, the World Health Organisation and the American Dietetic Association. However, some so-called ‘health’ organisations, health professionals and food writers persist in promoting red meat as the best source of iron. They invariably fail to mention the health risks
associated with the type of iron found in meat as opposed to iron from plants. This fact sheet debunks the Western myth of promoting meat as a good source of iron and explains why plant iron is best.
What is Iron and Why Do We Need It?
Iron is an essential component of the pigment haemoglobin, found in red blood cells. It helps carry oxygen to all parts of the body and is essential for life. If iron intake is low, the amount of haemoglobin in the red blood cells can fall leading to iron deficiency anaemia. Symptoms include tiredness, weakness, feeling cold and an inability to concentrate.
How Much Iron Do We Need?
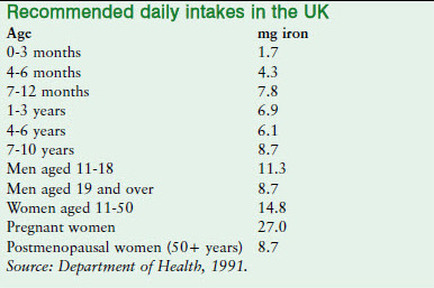
The UK recommended nutrient intake (RNI) for iron in adult males is 8.7 mg per day and for women up to the age of 50 it is 14.8 mg per day (Department of Health, 1991). Women have higher requirements as they lose iron during menstruation. The RNIs for younger and older groups are given below.
Supplements
Supplementing the diet with too much iron can lead to constipation, nausea, vomiting and stomach pain and very high doses can be fatal, particularly in children (FSA, 2003). Furthermore, not all supplements are the same. For example, iron (ferrous) sulphate (which many GPs prescribe) can cause nausea and constipation and may interfere with vitamin E absorption. However, other forms are much better-tolerated such as iron picolinate, iron citrate and iron bisglycinate. Plant forms of iron supplements such as Floradix and Floravital, sold in health food shops, are gentle on the system. The VVF recommends that you seek the advice of a nutritional therapist before taking supplements. Most people can get all the iron they need by eating a varied and balanced diet.
Types of Iron
There are two types of iron in food: Haem Iron is found in animal tissue. It is a component ofhaemoglobin (an oxygen-carrying protein in the blood) and myoglobin (oxygen-carrying molecules in muscle) and makes up around half the iron found in red meat, poultry and fish. Non-Haem Iron makes up the other half of the iron in animal tissue and all of the iron found in plant foods, dairy foods (which contain a very small amount) and eggs. Around 90 per cent of the iron in the average British diet is non-haem iron; the other 10 per cent comes mainly from the haemoglobin of meat (Bull and Buss, 1980). The UK’s Food Standards Agency (FSA) looked at sources of iron in their 2003 National Diet and Nutrition Survey and found that 17 per cent of total (haem and non-haem) iron came from meat, three per cent from fish, three from eggs and one per cent from dairy foods. The vast majority (over 75 per cent) of iron in the diet came from plant-based foods. Cereals (such as wholegrain pasta, brown rice and wholemeal bread) made the single biggest
contribution at 44 per cent (FSA, 2003a). This demonstrates the important contribution plant foods make to iron intake in meateaters and veggies alike.
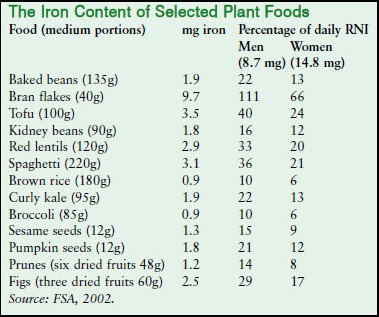
The Iron Content of Plant Foods
The table below shows that there is no shortage of iron in plant foods. Pulses (peas, beans and lentils) and soya bean products (such as soya milk and tofu) provide an excellent source. As do dark green leafy vegetables (such as broccoli, pak choy and watercress), fortified breakfast cereals, wholegrains (such as wholemeal bread, brown rice and wholemeal pasta), dried fruits (such as raisins, prunes, apricots and figs) black treacle and plaindark chocolate.
Supplementing the diet with too much iron can lead to constipation, nausea, vomiting and stomach pain and very high doses can be fatal, particularly in children (FSA, 2003). Furthermore, not all supplements are the same. For example, iron (ferrous) sulphate (which many GPs prescribe) can cause nausea and constipation and may interfere with vitamin E absorption. However, other forms are much better-tolerated such as iron picolinate, iron citrate and iron bisglycinate. Plant forms of iron supplements such as Floradix and Floravital, sold in health food shops, are gentle on the system. The VVF recommends that you seek the advice of a nutritional therapist before taking supplements. Most people can get all the iron they need by eating a varied and balanced diet.
Types of Iron
There are two types of iron in food: Haem Iron is found in animal tissue. It is a component ofhaemoglobin (an oxygen-carrying protein in the blood) and myoglobin (oxygen-carrying molecules in muscle) and makes up around half the iron found in red meat, poultry and fish. Non-Haem Iron makes up the other half of the iron in animal tissue and all of the iron found in plant foods, dairy foods (which contain a very small amount) and eggs. Around 90 per cent of the iron in the average British diet is non-haem iron; the other 10 per cent comes mainly from the haemoglobin of meat (Bull and Buss, 1980). The UK’s Food Standards Agency (FSA) looked at sources of iron in their 2003 National Diet and Nutrition Survey and found that 17 per cent of total (haem and non-haem) iron came from meat, three per cent from fish, three from eggs and one per cent from dairy foods. The vast majority (over 75 per cent) of iron in the diet came from plant-based foods. Cereals (such as wholegrain pasta, brown rice and wholemeal bread) made the single biggest
contribution at 44 per cent (FSA, 2003a). This demonstrates the important contribution plant foods make to iron intake in meateaters and veggies alike.
The Iron Content of Plant Foods
The table below shows that there is no shortage of iron in plant foods. Pulses (peas, beans and lentils) and soya bean products (such as soya milk and tofu) provide an excellent source. As do dark green leafy vegetables (such as broccoli, pak choy and watercress), fortified breakfast cereals, wholegrains (such as wholemeal bread, brown rice and wholemeal pasta), dried fruits (such as raisins, prunes, apricots and figs) black treacle and plaindark chocolate.
Iron Absorption
Both haem and non-haem iron are absorbed in the small intestine, but by different mechanisms. It is thought that haem iron is transported across the intestinal membrane (gut wall) into the blood intact where the iron component is removed to enter a common pool of iron along with non-haem iron (Geissler and Powers, 2005). This process occurs regardless of how much iron there already is in the body (iron status) and what else is in the diet. This is why haem iron is more easily absorbed than non-haem iron; estimates vary from 15-35 per cent for haem iron and two- 20 per cent for non-haem iron (Monsen, 1988). The amount of non-haem iron absorbed in the gut varies widely as it is subject to a range of influences including iron status and other foods present in the diet. A range of dietary factors influence nonhaem iron absorption. A high absorption rate is not necessarily a good thing as the body has no mechanism for disposing of excess iron. In other words, iron from plant foods is more beneficial to the body because its absorption remains safely regulated. Whereas iron from animal sources can accumulate to levels which could be harmful (see below).
Both haem and non-haem iron are absorbed in the small intestine, but by different mechanisms. It is thought that haem iron is transported across the intestinal membrane (gut wall) into the blood intact where the iron component is removed to enter a common pool of iron along with non-haem iron (Geissler and Powers, 2005). This process occurs regardless of how much iron there already is in the body (iron status) and what else is in the diet. This is why haem iron is more easily absorbed than non-haem iron; estimates vary from 15-35 per cent for haem iron and two- 20 per cent for non-haem iron (Monsen, 1988). The amount of non-haem iron absorbed in the gut varies widely as it is subject to a range of influences including iron status and other foods present in the diet. A range of dietary factors influence nonhaem iron absorption. A high absorption rate is not necessarily a good thing as the body has no mechanism for disposing of excess iron. In other words, iron from plant foods is more beneficial to the body because its absorption remains safely regulated. Whereas iron from animal sources can accumulate to levels which could be harmful (see below).
Factors that Decrease Iron Absorption
Phytate (inositol hexaphosphate) is found in unrefined grains, seeds and pulses (which are also a rich source of iron); bran is a particularly rich source. It is a strong binder of iron and other minerals (including calcium, magnesium and zinc) and can contribute to mineral deficiencies in people whose intake of these nutrients is low. For example, low iron absorption from porridge made from rice, maize, wheat, oat or sorghum, contributes to the high prevalence of iron deficiency in infants from Third World countries (Hurrell et al., 2003). There are various ways you can combat the effects of phytate. Eating foods rich in vitamin C with iron-rich food can help (see below). Also, cooking can increase the amount of iron available (Viadel et al., 2006; Bishnoi et al., 1994). One study showed that 37 out of 48 different vegetables provided more iron after being cooked (Yang et al., 2002). The available iron in broccoli increased five-fold and in cabbage, three-fold. Increasing the amount of time bread is fermented also lowers the phytate content (Nävert et al., 1985). Sprouting grains, seeds and pulses is another effective way of reducing phytate as it is released on germination. Studies show that germinating and dehusking can reduce phytate in rice and mung beans by 92 per cent (Marero et al., 1991), and increase iron absorption from various grains and pulses by between 20 and 62 per cent (Hemalatha et al., 2007). Remember though, wholemeal bread and brown rice contain around two to three times the amount of iron found in white bread and rice (Craig et al., 1994). So even though the percentage of iron absorbed from wholegrain foods may be lower, the total amount of iron absorbed is similar, making wholegrain foods the healthier option as they also contain more vitamins, minerals and fibre.
Polyphenols and Tannins
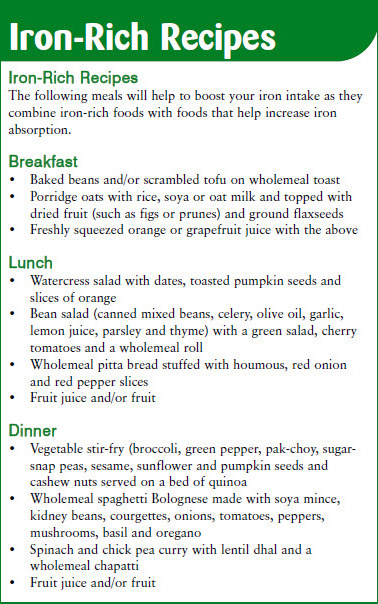
Polyphenols are a group of chemical substances found in plants that possess antioxidant properties that may offer potential health benefits such as a reduced risk of cardiovascular disease (CVD) and cancer. Tannins are a type of polyphenol found in tea and red wine that bind with non-haem iron to form complexes that may reduce iron absorption (Brune et al., 1989). The effect of tannins may be a concern for those who regularly consume wine with food. However, alcohol may enhance iron absorption (by stimulating gastric acid secretion) and some researchers conclude that the inhibitory effect of phenolic compounds in red wine is unlikely to affect iron balance significantly (Cook et al., 1995). There has been conflicting evidence on the effect of tea-drinking on iron status. However, the research appears to show that tea consumption does not influence iron status in healthy people who eat a well-balanced diet and have adequate iron stores (Temme and Hoydonck, 2002; Nelson and Poulter, 2004). If you are concerned about your iron levels and are used to drinking tea with meals (or just breakfast) try switching to freshly squeezed orange juice instead (because its vitamin C content increases the absorption of iron) and wait at least one hour after eating before drinking tea.
Calcium
Some studies show that serving cow’s milk with a meal can reduce iron absorption. This inhibitory effect is thought to be related to the milk protein casein (Hurrell et al., 1989) and calcium (Hallberg et al., 1991). Unlike phytate and tannin, calcium reduces non-haem and haem iron absorption (Fairweather-Tait, 2004) and this inhibitory effect is not negated by vitamin C or other acids. Calcium is thought to inhibit iron absorption by reducing phytate breakdown. In one study as little as 40 mg of calcium added to 80 grams of flour reduced phytate degradation by 50 per cent (Hallberg et al., 1991). Calcium also has a direct inhibitory effect on iron absorption. In the same study, giving 165 mg of calcium (as milk, cheese or calcium chloride) reduced iron absorption by 50-60 per cent. The authors concluded that the inhibitory effect of calcium in amounts frequently encountered in normal meals has important nutritional implications. This doesn’t mean you should limit your calcium intake; calcium is a very important mineral. However, to limit the negative effects of calcium on iron absorption avoid drinking cow’s milk and taking calcium supplements with food.
Oxalic Acid
Oxalic acid is a compound found in many plants such as spinach, Swiss chard and beetroot leaves. It also occurs in tea, chocolate and other cocoa products. It can bind with calcium and magnesium to form insoluble salts which reduce the absorption of these important minerals. Some work suggests that oxalic acid may also compromise iron absorption. However, recent evidence suggests that oxalic acid in fruits and vegetables is of minorrelevance in iron nutrition (Bonsmann et al., 2008).
Polyphenols are a group of chemical substances found in plants that possess antioxidant properties that may offer potential health benefits such as a reduced risk of cardiovascular disease (CVD) and cancer. Tannins are a type of polyphenol found in tea and red wine that bind with non-haem iron to form complexes that may reduce iron absorption (Brune et al., 1989). The effect of tannins may be a concern for those who regularly consume wine with food. However, alcohol may enhance iron absorption (by stimulating gastric acid secretion) and some researchers conclude that the inhibitory effect of phenolic compounds in red wine is unlikely to affect iron balance significantly (Cook et al., 1995). There has been conflicting evidence on the effect of tea-drinking on iron status. However, the research appears to show that tea consumption does not influence iron status in healthy people who eat a well-balanced diet and have adequate iron stores (Temme and Hoydonck, 2002; Nelson and Poulter, 2004). If you are concerned about your iron levels and are used to drinking tea with meals (or just breakfast) try switching to freshly squeezed orange juice instead (because its vitamin C content increases the absorption of iron) and wait at least one hour after eating before drinking tea.
Calcium
Some studies show that serving cow’s milk with a meal can reduce iron absorption. This inhibitory effect is thought to be related to the milk protein casein (Hurrell et al., 1989) and calcium (Hallberg et al., 1991). Unlike phytate and tannin, calcium reduces non-haem and haem iron absorption (Fairweather-Tait, 2004) and this inhibitory effect is not negated by vitamin C or other acids. Calcium is thought to inhibit iron absorption by reducing phytate breakdown. In one study as little as 40 mg of calcium added to 80 grams of flour reduced phytate degradation by 50 per cent (Hallberg et al., 1991). Calcium also has a direct inhibitory effect on iron absorption. In the same study, giving 165 mg of calcium (as milk, cheese or calcium chloride) reduced iron absorption by 50-60 per cent. The authors concluded that the inhibitory effect of calcium in amounts frequently encountered in normal meals has important nutritional implications. This doesn’t mean you should limit your calcium intake; calcium is a very important mineral. However, to limit the negative effects of calcium on iron absorption avoid drinking cow’s milk and taking calcium supplements with food.
Oxalic Acid
Oxalic acid is a compound found in many plants such as spinach, Swiss chard and beetroot leaves. It also occurs in tea, chocolate and other cocoa products. It can bind with calcium and magnesium to form insoluble salts which reduce the absorption of these important minerals. Some work suggests that oxalic acid may also compromise iron absorption. However, recent evidence suggests that oxalic acid in fruits and vegetables is of minorrelevance in iron nutrition (Bonsmann et al., 2008).
Factors that Increase Iron Absorption
Vitamin C
Vitamin C (ascorbic acid) found in abundance in fruit and vegetables, can increase the amount of iron absorbed considerably (Hunt et al., 1990; Sharma and Mathur, 1995). It does this by two mechanisms: converting iron into a soluble, more readily absorbable form and by binding to it, preventing it from forming complexes with phytate or tannin (Fairweather-Tait, 2004). The amount of vitamin C in eight strawberries or 200 ml of orange juice (75 mg) can increase iron absorption three- to four-fold (Craig, 1994). To increase your iron absorption substitute your morning cup of tea or coffee with a glass of freshly squeezed orange juice. If you are concerned about low iron levels, try to combine vitamin C-containing foods with your iron-rich meal. See suggestions below.
Meat
Small amounts of meat (around 50 grams) have been shown to increase non-haem iron absorption from meals that contain high levels of phytate and are low in vitamin C (Baech et al., 2003). Several groups have tried to identify the elusive ‘meat factor.’ Potential candidates include certain amino acids (the building blocks of protein) found in meat, which may convert non-haem iron into a more absorbable form. Alternatively, it may be a component of muscle tissue called L-alpha-glycerophosphocholine that helps (Armah et al., 2008). However, vitamin C seems to be a stronger enhancer of non-haem iron absorption than meat (Baech et al., 2003) and if vitamin C intake is adequate then meat may have little effect.
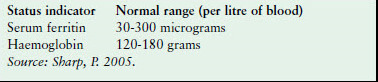
Measuring Iron Status
There are several different ways of assessing the body’s iron status. Two of the most common methods involve measuring haemoglobin and serum ferritin. Ferric is a term that means containing or having to do with iron, derived from the Latin word ferrum, meaning ‘iron’. Ferritin is a protein that stores iron for later use by your body. So the amount of ferritin in your blood reflects the amount of iron you have tucked away for future use. You can have normal haemoglobin levels, yet low ferritin. Ferritin levels are low in long-term iron deficiency, or if your body’s protein levels are very low, as in some cases of malnutrition. Conversely, ferritin levels are high in states of long-term iron overload. If you think that you might have too little (or too much) iron in your blood you can ask for a blood test. In the West, low iron levels and anaemia are usually due to long-term or heavy bleeding (in menstruation for example), pregnancy or rapid growth in children rather than a poor diet. High iron levels can be due to a genetic condition, extensive blood transfusions or an overdose of iron supplements.
Vitamin C
Vitamin C (ascorbic acid) found in abundance in fruit and vegetables, can increase the amount of iron absorbed considerably (Hunt et al., 1990; Sharma and Mathur, 1995). It does this by two mechanisms: converting iron into a soluble, more readily absorbable form and by binding to it, preventing it from forming complexes with phytate or tannin (Fairweather-Tait, 2004). The amount of vitamin C in eight strawberries or 200 ml of orange juice (75 mg) can increase iron absorption three- to four-fold (Craig, 1994). To increase your iron absorption substitute your morning cup of tea or coffee with a glass of freshly squeezed orange juice. If you are concerned about low iron levels, try to combine vitamin C-containing foods with your iron-rich meal. See suggestions below.
Meat
Small amounts of meat (around 50 grams) have been shown to increase non-haem iron absorption from meals that contain high levels of phytate and are low in vitamin C (Baech et al., 2003). Several groups have tried to identify the elusive ‘meat factor.’ Potential candidates include certain amino acids (the building blocks of protein) found in meat, which may convert non-haem iron into a more absorbable form. Alternatively, it may be a component of muscle tissue called L-alpha-glycerophosphocholine that helps (Armah et al., 2008). However, vitamin C seems to be a stronger enhancer of non-haem iron absorption than meat (Baech et al., 2003) and if vitamin C intake is adequate then meat may have little effect.
Measuring Iron Status
There are several different ways of assessing the body’s iron status. Two of the most common methods involve measuring haemoglobin and serum ferritin. Ferric is a term that means containing or having to do with iron, derived from the Latin word ferrum, meaning ‘iron’. Ferritin is a protein that stores iron for later use by your body. So the amount of ferritin in your blood reflects the amount of iron you have tucked away for future use. You can have normal haemoglobin levels, yet low ferritin. Ferritin levels are low in long-term iron deficiency, or if your body’s protein levels are very low, as in some cases of malnutrition. Conversely, ferritin levels are high in states of long-term iron overload. If you think that you might have too little (or too much) iron in your blood you can ask for a blood test. In the West, low iron levels and anaemia are usually due to long-term or heavy bleeding (in menstruation for example), pregnancy or rapid growth in children rather than a poor diet. High iron levels can be due to a genetic condition, extensive blood transfusions or an overdose of iron supplements.
Iron Deficiency
A lack of iron in the body is the most common nutritional problem worldwide (Sharp, 2005). In fact a quarter of the world’s population may be iron deficient and approximately 500 million people suffer from iron deficiency anaemia (Cook et al., 1994). Symptoms include fatigue, pale skin and a weakened immune system. A reduced ability to concentrate can also lead to problems at school for children with iron deficiency anaemia (Grantham- McGregor and Ani, 2001). The FSA states that groups that are vulnerable to iron deficiency include: infants over six months, toddlers, adolescents and pregnant women because of their increased requirements (FSA, 2003). Older people and those consuming foods that inhibit iron absorption may suffer due to poor absorption. Menstruating women and individuals with pathological blood loss may also be at risk due to high blood losses. For example, one study looking at menstrual blood loss and diet among women in the UK concluded that menstrual blood loss was the most significant factor affecting iron status, although the type of diet did affect iron stores (Harvey et al., 2005). The FSA does not identify vegetarians and vegans as a vulnerable group.
A lack of iron in the body is the most common nutritional problem worldwide (Sharp, 2005). In fact a quarter of the world’s population may be iron deficient and approximately 500 million people suffer from iron deficiency anaemia (Cook et al., 1994). Symptoms include fatigue, pale skin and a weakened immune system. A reduced ability to concentrate can also lead to problems at school for children with iron deficiency anaemia (Grantham- McGregor and Ani, 2001). The FSA states that groups that are vulnerable to iron deficiency include: infants over six months, toddlers, adolescents and pregnant women because of their increased requirements (FSA, 2003). Older people and those consuming foods that inhibit iron absorption may suffer due to poor absorption. Menstruating women and individuals with pathological blood loss may also be at risk due to high blood losses. For example, one study looking at menstrual blood loss and diet among women in the UK concluded that menstrual blood loss was the most significant factor affecting iron status, although the type of diet did affect iron stores (Harvey et al., 2005). The FSA does not identify vegetarians and vegans as a vulnerable group.
Veggie Diets and Iron
Vegetarian diets have been described as being deficient in iron, although numerous studies show that when this occurs, it is usually due to poor meal planning (Leitzmann, 2005). A well-balanced vegetarian or vegan diet provides plenty of iron. In fact, in Western countries, vegetarian diets can contain as much or more iron than mixed diets containing meat (Harvey et al., 2005; Hunt, 2003). Vegetarians and vegans, even with a high dietary fibre (and hence phytate) intake, have been found to have a similar amount of iron in their diets compared to meat-eaters (Craig, 1994). A recent study compared iron intake among 33,000 meat-eaters, 10,000 fish-eaters, 18,000 vegetarians and 2,500 vegans and found that the vegans had the highest intake, followed by the fish-eaters and the vegetarians; the meat-eaters had the lowest intake (Davey, et al., 2003).
Vegetarians tend to have lower iron stores (serum ferritin) than meat-eaters. This may be because haem iron is more readily absorbed than non-haem iron, because meat enhances non-haem iron absorption or because vegetarian diets may contain higher levels of inhibitors of iron absorption such as phytate, tannins and calcium (Harvey et al., 2005). However, vegetarians have no greater incidence of iron deficiency anaemia. The British Medical Association and the American Dietetic Association agree that vegetarians are no more likely to suffer from iron deficiency than meat eaters (BMA, 1986; American Dietetic Association, 2003). Although vegetarians have lower iron stores, adverse health effects have not been demonstrated with varied vegetarian diets in developed countries. In fact, moderately lower iron stores reduce the risk of some chronic diseases (Hunt, 2003). It is well known that many meat eaters are oversupplied with iron, increasing the risk of cardiovascular disease (CVD) and certain cancers (Leitzmann, 2005).
Too Much of a Good Thing?
Excessive iron in the body is toxic. Despite this, there exists a widespread conviction that the more iron in the diet the better. This is what is still written in some nutrition and dietetic textbooks. Numerous studies now show that people with high iron stores suffer a higher incidence of cardiovascular disease (CVD), certain cancers and other health problems. Iron overload can be caused by an inherited genetic condition (hereditary haemochromatosis), which affects one in 250 people (of Northern European descent) (Burke et al., 2000). Normally the liver stores a small amount of iron to provide new red blood cells with it. If you absorb excessive amounts of iron (as some people with this condition do) it builds up in the liver and is deposited in other tissues and organs. Iron overload may cause uncomfortable symptoms such as nausea, abdominal pain, constipation and joint pain. It can also lead to liver damage, heart failure and diabetes (NHS Direct, 2008). Men are more at risk from haemochromatosis because women regularly lose blood (and therefore iron), during menstruation. This condition illustrates how you can have too much of a good thing.
Iron and Heart Disease
The idea that high iron stores can increase the risk of heart disease was first proposed in the Lancet in 1981 (Sullivan, 1981). Sullivan proposed that menstrual blood loss could be responsible for the lower risk of heart disease observed among pre-menstrual women compared to men of the same age. Since then, other studies have confirmed that high iron stores are a risk factor for CVD (Salonen et al., 1992). As well as menstruation in women, voluntary blood donation is an important cause of blood loss that can affect iron stores. In 1997, three different studies showed that regular blood donation reduced the risk of heart disease and strokes (Tuomainen et al., 1997; Meyers et al., 1997; Kiechl et al., 1997). The loss of iron associated with giving blood could be the reason for the observed reduction in risk. More recently another study showed that high frequency blood donation was associated with lower iron stores, improved vascular function and reduced oxidative stress in blood donors (Zheng et al., 2005). The theory is that iron promotes the production of harmful molecules called free radicals that can cause (oxidative) damage to the lining of the arteries. This, in turn, increases the risk of CVD. These findings lend further support to the hypothesis linking high iron stores to CVD. However, some studies have concluded that there is no association between iron status and CVD. In a letter to the British Medical Journal, researchers from Finland countered this argument by asserting that all of the negative studies used unreliable measurements of iron status (such as serum iron concentration, transferrin iron saturation) or other design problem (Hemilä and Paunio, 1997).So convinced of the link are some researchers that they have suggested reducing iron stores to reduce the risk of CVD. Some say the evidence may even be strong enough to recommend ending iron fortification and supplementation and to start advising people to donate blood to reduce their stores of iron. However, others caution that, given the extent of iron deficiency, any decision to reverse iron fortification and supplementation policy should be based on extremely sound science (Sempos, 2002). Clearly more research is needed. The sensible approach is to eat a well-balanced vegetarian or vegan diet containing plenty of iron-rich plant-based foods.
Iron and Diabetes
Up to 65 per cent of patients with haemochromatosis develop diabetes (Adams et al., 1991). As people with this condition accumulate iron stores in the body, this has led to speculation that iron overload may cause diabetes. An investigation into iron intake and diabetes revealed that while total iron intake was not related to diabetes, haem-iron intake from red meat was (Jiang et al., 2004). Haem-iron is absorbed in an unregulated way and so accumulates in the body over time. As stated above, iron can catalyse the formation of free radicals. These harmful molecules are implicated in the development of diabetes (Oberley, 1988; Wolff, 1993) and other diseases. New research also indicates an association between high iron status in pregnant women and gestational diabetes. The authors of this study conclude that the role of iron excess from iron supplementation in the development of gestational diabetes needs to be examined (Afkhami-Ardekani and Rashidi, 2008). Taken together, the research indicates that insulin resistance and diabetes is directly related to excessive iron stores. The good news is that vegetarians and vegans have less insulin resistance and diabetes than meat-eaters (Kuo et al., 2004). Remember, a vegan diet provides iron in its non-haem form, which is absorbed in a more regulated way than haem-iron. A study comparing 30 vegetarians and 30 meat-eaters showed that vegetarians had adequate but lower body iron stores compared with meat-eaters. The vegetarians also had less insulin resistance (Hua et al., 2001). In summary, vegetarians and vegans tend to have lower iron stores than meat-eaters, but have no greater incidence of iron deficiency anaemia. Conversely, it is well known that many meat-eaters are oversupplied with iron, increasing the risk of CVD and cancer (Leitzmann, 2005).
Baby Blues
For the first six months of life, infants require only breast milk, which contains appropriate amounts of iron (or specially formulated milk). At around six months of age their nutritional requirements increase and they need more than milk alone. For example, the daily iron requirement of an infant rises from 4.3mg at four to six months, to 7.8mg at six months. A primary cause of anaemia in infants is therefore inappropriate weaning – too early, too late or an unbalanced diet. To make matters worse, cow’s milk allergy can lead to gastrointestinal bleeding and is a well-recognised cause of rectal bleeding in infancy (Willetts et al., 1999). Gastrointestinal bleeding from milk allergy often occurs in such small quantities that the blood loss is not noticed, but over time these losses can cause iron deficiency anaemia in infants. In a trial of 52 infants (31 of whom had been breast fed and 21 fed formula milk), the introduction of cow’s milk rather than formula milk was associated with an increased blood loss from the intestinal tract and a nutritionally important loss of iron (Ziegler et al., 1990). Frank Oski, former paediatrics director at Johns Hopkins School of Medicine, estimates that half the iron deficiency in infants in the US results from cow’s milk-induced gastrointestinal bleeding (Oski, 1996). This represents a staggering figure since more than 15 per cent of US infants under the age of two suffer from iron deficiency anaemia.
The idea that high iron stores can increase the risk of heart disease was first proposed in the Lancet in 1981 (Sullivan, 1981). Sullivan proposed that menstrual blood loss could be responsible for the lower risk of heart disease observed among pre-menstrual women compared to men of the same age. Since then, other studies have confirmed that high iron stores are a risk factor for CVD (Salonen et al., 1992). As well as menstruation in women, voluntary blood donation is an important cause of blood loss that can affect iron stores. In 1997, three different studies showed that regular blood donation reduced the risk of heart disease and strokes (Tuomainen et al., 1997; Meyers et al., 1997; Kiechl et al., 1997). The loss of iron associated with giving blood could be the reason for the observed reduction in risk. More recently another study showed that high frequency blood donation was associated with lower iron stores, improved vascular function and reduced oxidative stress in blood donors (Zheng et al., 2005). The theory is that iron promotes the production of harmful molecules called free radicals that can cause (oxidative) damage to the lining of the arteries. This, in turn, increases the risk of CVD. These findings lend further support to the hypothesis linking high iron stores to CVD. However, some studies have concluded that there is no association between iron status and CVD. In a letter to the British Medical Journal, researchers from Finland countered this argument by asserting that all of the negative studies used unreliable measurements of iron status (such as serum iron concentration, transferrin iron saturation) or other design problem (Hemilä and Paunio, 1997).So convinced of the link are some researchers that they have suggested reducing iron stores to reduce the risk of CVD. Some say the evidence may even be strong enough to recommend ending iron fortification and supplementation and to start advising people to donate blood to reduce their stores of iron. However, others caution that, given the extent of iron deficiency, any decision to reverse iron fortification and supplementation policy should be based on extremely sound science (Sempos, 2002). Clearly more research is needed. The sensible approach is to eat a well-balanced vegetarian or vegan diet containing plenty of iron-rich plant-based foods.
Iron and Diabetes
Up to 65 per cent of patients with haemochromatosis develop diabetes (Adams et al., 1991). As people with this condition accumulate iron stores in the body, this has led to speculation that iron overload may cause diabetes. An investigation into iron intake and diabetes revealed that while total iron intake was not related to diabetes, haem-iron intake from red meat was (Jiang et al., 2004). Haem-iron is absorbed in an unregulated way and so accumulates in the body over time. As stated above, iron can catalyse the formation of free radicals. These harmful molecules are implicated in the development of diabetes (Oberley, 1988; Wolff, 1993) and other diseases. New research also indicates an association between high iron status in pregnant women and gestational diabetes. The authors of this study conclude that the role of iron excess from iron supplementation in the development of gestational diabetes needs to be examined (Afkhami-Ardekani and Rashidi, 2008). Taken together, the research indicates that insulin resistance and diabetes is directly related to excessive iron stores. The good news is that vegetarians and vegans have less insulin resistance and diabetes than meat-eaters (Kuo et al., 2004). Remember, a vegan diet provides iron in its non-haem form, which is absorbed in a more regulated way than haem-iron. A study comparing 30 vegetarians and 30 meat-eaters showed that vegetarians had adequate but lower body iron stores compared with meat-eaters. The vegetarians also had less insulin resistance (Hua et al., 2001). In summary, vegetarians and vegans tend to have lower iron stores than meat-eaters, but have no greater incidence of iron deficiency anaemia. Conversely, it is well known that many meat-eaters are oversupplied with iron, increasing the risk of CVD and cancer (Leitzmann, 2005).
Baby Blues
For the first six months of life, infants require only breast milk, which contains appropriate amounts of iron (or specially formulated milk). At around six months of age their nutritional requirements increase and they need more than milk alone. For example, the daily iron requirement of an infant rises from 4.3mg at four to six months, to 7.8mg at six months. A primary cause of anaemia in infants is therefore inappropriate weaning – too early, too late or an unbalanced diet. To make matters worse, cow’s milk allergy can lead to gastrointestinal bleeding and is a well-recognised cause of rectal bleeding in infancy (Willetts et al., 1999). Gastrointestinal bleeding from milk allergy often occurs in such small quantities that the blood loss is not noticed, but over time these losses can cause iron deficiency anaemia in infants. In a trial of 52 infants (31 of whom had been breast fed and 21 fed formula milk), the introduction of cow’s milk rather than formula milk was associated with an increased blood loss from the intestinal tract and a nutritionally important loss of iron (Ziegler et al., 1990). Frank Oski, former paediatrics director at Johns Hopkins School of Medicine, estimates that half the iron deficiency in infants in the US results from cow’s milk-induced gastrointestinal bleeding (Oski, 1996). This represents a staggering figure since more than 15 per cent of US infants under the age of two suffer from iron deficiency anaemia.
|
Summary
• Iron is an essential part of the haemoglobin in red blood cells which helps carry oxygen to all parts of the body. • The UK recommended nutrient intake for iron in adult males is 8.7 mg per day and for women up to 50 it is 14.8 mg per day. • Most people can get all the iron they need by eating a varied and balanced diet. • Too much iron can lead to constipation, nausea, vomiting and stomach pain and very high doses can be fatal, particularly in children. • Ferrous sulphate as a supplement can lead to constipation and nausea. • There are two types of iron in food: haem iron from meat and non-haem iron from plant foods. • Most iron in the diet (over 75 per cent) comes from plantbased foods. • Good sources of iron include pulses (peas, beans and lentils), soya bean products (soya milk and tofu), dark green leafy vegetables (parsley, broccoli, pak choy and watercress), fortified breakfast cereals, wholegrains (wholemeal bread, wholemeal pasta), dried fruits (raisins, prunes, apricots and figs) black treacle and plain dark chocolate. • Haem iron is absorbed regardless of both iron status and what else is in the diet. • Non-haem iron absorption is subject to a range of influences including iron status and other foods in the diet. • Iron from animal sources and supplements can accumulate to harmful levels. • Phytate from unrefined grains, seeds and pulses binds iron and can reduce absorption. Phytate can be reduced by fermenting, cooking and sprouting.• Tannins in tea may reduce iron absorption. Avoid drinking tea with meals. • Cow’s milk (casein and calcium) can reduce iron absorption. Avoid drinking cow’s milk and taking calcium supplements with food. • Oxalic acid in spinach, Swiss chard and beetroot is of minor relevance in iron nutrition. |
Soya protein may decrease iron absorption although this effect
can be reduced by lowering the amount of phytate present. • Vitamin C in fruit and vegetables can increase iron absorption considerably; the amount of vitamin C in 200 ml of orange juice can increase iron absorption three- to four-fold.• Small amounts of meat may increase non-haem iron absorption from high-phytate, low-vitamin C meals that contain high levels of phytate, but vitamin C is a stronger enhancer of nonhaem iron absorption than meat. • Iron status is assessed by measuring haemoglobin and serum ferritin. • In the West, low iron levels and anaemia are usually due to long-term or heavy bleeding (in menstruation for example), pregnancy or rapid growth in children rather than a poor diet. • High iron levels can be due to a genetic condition, extensive blood transfusions or (more rarely) an overdose of iron supplements. • Low iron in the body is the most common nutritional problem worldwide. Symptoms include fatigue, pale skin, a weakened immune system and a reduced ability to concentrate. • Vulnerable groups include: infants over six months, toddlers, adolescents and pregnant as well as older people and those consuming foods that inhibit iron absorption. Menstruating women and people with pathological blood loss may also be at risk. • A well-balanced vegetarian or vegan diet provides as much or more iron than mixed diets containing meat. • Vegetarians tend to have lower iron stores than meat-eaters but have no greater incidence of iron deficiency anaemia. • Moderately lower iron stores may reduce the risk of some chronic diseases. • Excessive iron in the body is toxic; symptoms include nausea, abdominal pain, constipation and joint pain. It can also lead to liver damage, heart failure and diabetes. • High iron stores may be a risk factor for CVD, insulin resistance and diabetes. • Anaemia in infants may be caused by inappropriate weaning orcow’s milk allergy induced gastrointestinal bleeding. |
Why Plant Calcium is Best

Most people in developed countries have been brought up to believe that our teeth and our bones can only grow healthily if we drink cow’s milk. Over the last three decades we have witnessed a barrage of marketing campaigns designed to reinforce the idea that only milk can supply calcium in sufficient quantities to help us grow big and strong. But is milk really good for you? An increasing amount of research challenges the outdated notion that cow’s milk is best and in fact shows that our consumption of dairy products is doing us much more harm than good.
What is Calcium and Why Do We Need It?
Calcium is a soft grey metallic element. It is the fifth most abundant element on the earth’s crust and occurs in compounds such as limestone, chalk and marble. Calcium is required for normal growth and development in animals. It is the most abundant mineral in the human body accounting for around two per cent of the total body weight. Calcium plays an important structural role in maintaining bone health and strength, in fact around 99 per cent of our calcium is deposited in the bones and teeth. The other one per cent is responsible for a range of important metabolic functions that regulate muscle contraction, heart beat, blood clotting and functioning of the nervous system.
How Much Calcium Do We Need?
There is no international consensus on what the healthiest or safest amount of calcium we need is. In the UK, the reference nutrient intake value (RNI) is used; this is similar to the Recommended Daily Amount (RDA) used previously. The RNI value for a nutrient is the amount of that nutrient that is sufficient for 97.5 per cent of the people in a given group. The UK government currently suggests that the RNI value for calcium in adults aged between 19 and 50 years of age is 700 mg per day In the US, the recommended daily intake is slightly higher at 1000mg per day However, in many countries such as India, China, Japan, Gambia and Peru the average daily intake of calcium can be as low as 300 mg.
Where Do We Get It?
The body obtains calcium in two ways, either from our diet or our bones. When the diet does not provide sufficient levels, calcium is borrowed’ (reabsorbed) from the bones in order to restore blood levels and maintain calcium-dependent biological functions. Calcium in our bones is reabsorbed and replaced continuously as old bone cells break down and new ones form. If adequate calcium is then supplied in the diet, bone levels are restored, but if the diet fails to supply enough calcium, bone loss persists.
The body obtains calcium in two ways, either from our diet or our bones. When the diet does not provide sufficient levels, calcium is borrowed’ (reabsorbed) from the bones in order to restore blood levels and maintain calcium-dependent biological functions. Calcium in our bones is reabsorbed and replaced continuously as old bone cells break down and new ones form. If adequate calcium is then supplied in the diet, bone levels are restored, but if the diet fails to supply enough calcium, bone loss persists.
Children, Young Adults and Bone Health
The idea that cow’s milk is the best source of calcium is deeply entrenched in the British psyche and is sustained by the government-sponsored dairy industry and Milk Development Council who work with schools, dairies and LEAs to encourage more children to drink milk at school. However, a recent review on dairy products and bone health published in the official journal of the American Academy of Pediatrics challenged this misleading notion by concluding that there is very little evidence to support increasing the consumption of dairy products in children and young adults in order to promote bone health This review examined the effects of dairy products and total dietary calcium on bone integrity in children and young adults and found that out of 37 studies, 27 showed no relationship between dairy or dietary calcium intake and measures of bone health. In the remaining studies the effects on bone health were either small or results were confounded by the fortification of milk with vitamin D. An increasing amount of evidence now suggests that milk is not the best source of calcium at all and goes further to suggest that our bone health would benefit enormously if we switched to plant-based sources. In addition, research suggests that physical exercise is the most critical factor for maintaining healthy bones, followed by improving the diet and lifestyle; this means eating plenty of fresh fruit and vegetables, and for young adults cutting down on caffeine and avoiding alcohol and smoking. In 2004 the Government’s Food Standards Agency (FSA) looked at sources of calcium in the National Diet and Nutrition Survey and found that only 43 per cent of the mean intake of calcium in adults in the UK comes from milk and milk products (1). So despite the misconceived notion that milk is the best (or only) source of calcium the facts show that a large share of the calcium in our diets is derived from sources other than dairy foods. This is not surprising as most people in the world (around 70 per cent) obtain their calcium from plant-based sources rather than dairy products. But Milk is a Natural Food… Isn’t It? Humans are mammals, and as with all mammals, we are designed to drink the milk of our mothers until we are weaned onto solid foods. We are the only mammals that continue to drink milk after weaning, and not just that, we are the only mammals to drink the milk of another species (apart from pets that we control). To state the obvious (but often overlooked fact) cow’s milk has evolved to help turn a small calf into a cow in less than a year. That’s why cow’s milk contains around four times as much calcium as human milk; 118mg per 100g compared to 34mg per 100g respectively This discrepancy is for a good reason; calves need a huge amount of calcium to promote the massive level of skeletal growth required over the first year of life. A human infant does not require such high levels of calcium; indeed the high mineral content of cow’s milk puts a strain on the human infant kidney which is why most governments recommend children do not drink cow’s milk in their first year. Indeed the mineral content of cow’s milk is so out of balance with human biochemistry that it is difficult for human adults to absorb the optimum amounts required for health.
The idea that cow’s milk is the best source of calcium is deeply entrenched in the British psyche and is sustained by the government-sponsored dairy industry and Milk Development Council who work with schools, dairies and LEAs to encourage more children to drink milk at school. However, a recent review on dairy products and bone health published in the official journal of the American Academy of Pediatrics challenged this misleading notion by concluding that there is very little evidence to support increasing the consumption of dairy products in children and young adults in order to promote bone health This review examined the effects of dairy products and total dietary calcium on bone integrity in children and young adults and found that out of 37 studies, 27 showed no relationship between dairy or dietary calcium intake and measures of bone health. In the remaining studies the effects on bone health were either small or results were confounded by the fortification of milk with vitamin D. An increasing amount of evidence now suggests that milk is not the best source of calcium at all and goes further to suggest that our bone health would benefit enormously if we switched to plant-based sources. In addition, research suggests that physical exercise is the most critical factor for maintaining healthy bones, followed by improving the diet and lifestyle; this means eating plenty of fresh fruit and vegetables, and for young adults cutting down on caffeine and avoiding alcohol and smoking. In 2004 the Government’s Food Standards Agency (FSA) looked at sources of calcium in the National Diet and Nutrition Survey and found that only 43 per cent of the mean intake of calcium in adults in the UK comes from milk and milk products (1). So despite the misconceived notion that milk is the best (or only) source of calcium the facts show that a large share of the calcium in our diets is derived from sources other than dairy foods. This is not surprising as most people in the world (around 70 per cent) obtain their calcium from plant-based sources rather than dairy products. But Milk is a Natural Food… Isn’t It? Humans are mammals, and as with all mammals, we are designed to drink the milk of our mothers until we are weaned onto solid foods. We are the only mammals that continue to drink milk after weaning, and not just that, we are the only mammals to drink the milk of another species (apart from pets that we control). To state the obvious (but often overlooked fact) cow’s milk has evolved to help turn a small calf into a cow in less than a year. That’s why cow’s milk contains around four times as much calcium as human milk; 118mg per 100g compared to 34mg per 100g respectively This discrepancy is for a good reason; calves need a huge amount of calcium to promote the massive level of skeletal growth required over the first year of life. A human infant does not require such high levels of calcium; indeed the high mineral content of cow’s milk puts a strain on the human infant kidney which is why most governments recommend children do not drink cow’s milk in their first year. Indeed the mineral content of cow’s milk is so out of balance with human biochemistry that it is difficult for human adults to absorb the optimum amounts required for health.
Lactose Intolerance
Many people are unable to consume cow’s milk and milk products because they are unable to digest the sugar in milk called lactose. This sugar only exists in mammals’ milk, including human breast milk. In order for lactose to be digested it must be broken down in the small intestine by the enzyme lactase. Most infants possess the enzyme lactase, and can therefore digest lactose, but this ability is lost in many people after weaning
(commonly after the age of two). Losing the ability to digest lactose at this age is a clear indication of how humans are not designed to drink milk as adults; it is not a natural food for us. The frequency of lactose intolerance varies from around 90-100 per cent of Asians, 65-70 per cent of Africans, to 10 per cent of Caucasians In the absence of lactase, lactose is fermented by bacteria in the large intestine, this leads to a build up of gas. Symptoms of lactose intolerance include nausea, cramps, bloating, wind, and diarrhoea. The treatment is straightforward: avoid lactose. This means cutting out all dairy foods and checking labels for lactose in bread, chocolate and other processed foods. Many lactose intolerant people obtain their calcium from plant-based sources.
Allergies
An allergic reaction to cow’s milk is very different to lactose intolerance and can, in extreme circumstances, be fatal. An allergic reaction to milk occurs when the body’s immune system perceives one of the proteins in milk (either whey or casein) as a foreign invader and launches an attack. Symptoms are generally more extreme than in lactose intolerance and include excessive mucus production resulting in a runny nose and blocked ears. More serious symptoms include eczema, colic, diarrhoea, asthma and vomiting. Casein is more difficult to avoid as it is commonly used in the production of bread, processed cereals, instant soups, margarine, salad dressings, sweets and cake mix. People with milk allergies tend to obtain their calcium from plant-based sources.
Cow’s Milk and Diabetes
Type I diabetes is an autoimmune disease where the immune system’s ‘soldiers’, known as T-cells, destroy the body’s own insulin-producing beta cells in the pancreas. This type of response is thought to involve a genetic predisposition (diabetes in the family) coupled to an environmental trigger such as cow insulin or casein – both from cow’s milk. Research shows that some infants may be more vulnerable to type I diabetes later in life if exposed to cow's milk formula while very young. A Finnish study of children (with at least one close relative with type I diabetes) examined
whether early exposure to insulin in cow’s milk formula increased the risk of type I diabetes. Results showed that infants given cow's milk formula at three months old had immune systems which reacted far more strongly to cow’s insulin This raises concerns that exposure to cow’s insulin plays a role in the autoimmune process leading to type I diabetes. Another environmental trigger in cow’s milk is thought to be a protein called casein Casein is similar in shape to the insulin producing cells in the pancreas. Because the body may see casein as a foreign invader and attack it, it may also start to attack the pancreas cells having confused them for casein; again leading to diabetes. A review of the clinical evidence suggests that the incidence of type I diabetes is related to the early consumption of cow’s milk; children with type I diabetes were more likely to have been breastfed for less than three months and to have been exposed to cow’s milk protein before four months of age. The avoidance of cow’s milk during the first few months of life may reduce the risk of type I diabetes. Infants who cannot breastfeed from their mothers would benefit more from taking a plant-based formula such as soya-based formula rather than one based on cow’s milk.
Many people are unable to consume cow’s milk and milk products because they are unable to digest the sugar in milk called lactose. This sugar only exists in mammals’ milk, including human breast milk. In order for lactose to be digested it must be broken down in the small intestine by the enzyme lactase. Most infants possess the enzyme lactase, and can therefore digest lactose, but this ability is lost in many people after weaning
(commonly after the age of two). Losing the ability to digest lactose at this age is a clear indication of how humans are not designed to drink milk as adults; it is not a natural food for us. The frequency of lactose intolerance varies from around 90-100 per cent of Asians, 65-70 per cent of Africans, to 10 per cent of Caucasians In the absence of lactase, lactose is fermented by bacteria in the large intestine, this leads to a build up of gas. Symptoms of lactose intolerance include nausea, cramps, bloating, wind, and diarrhoea. The treatment is straightforward: avoid lactose. This means cutting out all dairy foods and checking labels for lactose in bread, chocolate and other processed foods. Many lactose intolerant people obtain their calcium from plant-based sources.
Allergies
An allergic reaction to cow’s milk is very different to lactose intolerance and can, in extreme circumstances, be fatal. An allergic reaction to milk occurs when the body’s immune system perceives one of the proteins in milk (either whey or casein) as a foreign invader and launches an attack. Symptoms are generally more extreme than in lactose intolerance and include excessive mucus production resulting in a runny nose and blocked ears. More serious symptoms include eczema, colic, diarrhoea, asthma and vomiting. Casein is more difficult to avoid as it is commonly used in the production of bread, processed cereals, instant soups, margarine, salad dressings, sweets and cake mix. People with milk allergies tend to obtain their calcium from plant-based sources.
Cow’s Milk and Diabetes
Type I diabetes is an autoimmune disease where the immune system’s ‘soldiers’, known as T-cells, destroy the body’s own insulin-producing beta cells in the pancreas. This type of response is thought to involve a genetic predisposition (diabetes in the family) coupled to an environmental trigger such as cow insulin or casein – both from cow’s milk. Research shows that some infants may be more vulnerable to type I diabetes later in life if exposed to cow's milk formula while very young. A Finnish study of children (with at least one close relative with type I diabetes) examined
whether early exposure to insulin in cow’s milk formula increased the risk of type I diabetes. Results showed that infants given cow's milk formula at three months old had immune systems which reacted far more strongly to cow’s insulin This raises concerns that exposure to cow’s insulin plays a role in the autoimmune process leading to type I diabetes. Another environmental trigger in cow’s milk is thought to be a protein called casein Casein is similar in shape to the insulin producing cells in the pancreas. Because the body may see casein as a foreign invader and attack it, it may also start to attack the pancreas cells having confused them for casein; again leading to diabetes. A review of the clinical evidence suggests that the incidence of type I diabetes is related to the early consumption of cow’s milk; children with type I diabetes were more likely to have been breastfed for less than three months and to have been exposed to cow’s milk protein before four months of age. The avoidance of cow’s milk during the first few months of life may reduce the risk of type I diabetes. Infants who cannot breastfeed from their mothers would benefit more from taking a plant-based formula such as soya-based formula rather than one based on cow’s milk.
Plant-Based Sources of Calcium
There are many plant-based sources of calcium. Good sources include non-oxalate (see below) dark green leafy vegetables such as broccoli, kale, spring greens, cabbage, bok choy, parsley and watercress. Also rich in calcium are dried fruits, such as figs and dates, nuts, particularly almonds and brazil nuts, and seeds including sesame seeds and tahini (sesame seed paste) which contains a massive 680 milligrams of calcium per 100 grams. Pulses including soya beans, kidney beans, chick peas, baked beans, broad beans, lentils, peas and calcium-set tofu (soya bean curd) provide a good source of calcium. Other fruit and vegetable sources include parsnips, swede, turnips, lemons, oranges, olives and molasses. A good additional source is calcium-enriched soya milk.
There are many plant-based sources of calcium. Good sources include non-oxalate (see below) dark green leafy vegetables such as broccoli, kale, spring greens, cabbage, bok choy, parsley and watercress. Also rich in calcium are dried fruits, such as figs and dates, nuts, particularly almonds and brazil nuts, and seeds including sesame seeds and tahini (sesame seed paste) which contains a massive 680 milligrams of calcium per 100 grams. Pulses including soya beans, kidney beans, chick peas, baked beans, broad beans, lentils, peas and calcium-set tofu (soya bean curd) provide a good source of calcium. Other fruit and vegetable sources include parsnips, swede, turnips, lemons, oranges, olives and molasses. A good additional source is calcium-enriched soya milk.
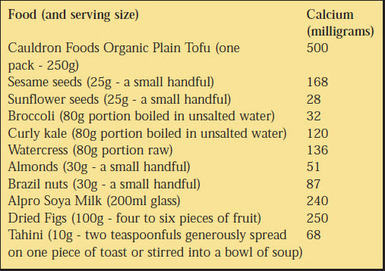
Calcium Uptake and Absorption
The amount of calcium present in a particular food is not the only important, factor to consider. The bioavailability of the calcium should be considered when deciding which foods are a good source. This means how much calcium is actually available for absorption into the body from the food. The calcium in dairy products is not as well absorbed as that in many dark green leafy vegetables For example, calcium absorbability from kale was demonstrated to be considerably higher than that from cow’s milk While spinach contains a relatively high amount of calcium, it is bound to a substance called oxalate which hinders calcium absorption so it is important to obtain calcium from low-oxalate green vegetables. Grains, nuts and seeds contain a substance called phytic acid which until recently was also considered to hinder calcium absorption, now phytic acid is believed to have only a minor influence Caffeine and smoking have been shown to reduce calcium absorption.
Vitamin D
The body requires vitamin D to absorb and retain calcium in the bones. Vitamin D is either obtained from the diet or it is synthesised in the skin following exposure to sunlight. But recent concerns about skin cancer have encouraged us to cover up and avoid the sun. Subsequently people in the UK could be at risk of vitamin D deficiency if they get too little sun exposure year round Without sufficient vitamin D, calcium deficiency is likely to occur even if the diet provides enough calcium. The consequences may be serious, resulting in rickets or osteomalacia (softening of the bones). Over the last few years there have been cases of vitamin D deficiency in some large UK cities Vegans obtain vitamin D from sunlight and fortified foods such as soya milks, cereals and margarines. It is important to get the balance right between being cautious about exposure to the sun and aware of the need for some exposure. It is now advised by the UK government that we apply sun block after 10 to 15 minutes exposure to the sun, this is so that we can synthesise vitamin D in the skin.
Magnesium, Potassium, Vitamin C and Vitamin K
Magnesium, potassium, vitamin C and vitamin K are all required for good bone health. A healthy diet that includes at least five servings a day of
fruit and vegetables should optimise the intake of these and other micronutrients required.
Animal Protein and Osteoporosis
Bones consist of a thick outer shell and a strong inner mesh filled with a protein called collagen, calcium salts and other minerals. Osteoporosis (meaning porous bones) occurs when calcium is lost from the bones and they become more fragile and prone to fracture. This debilitating condition tends to occur mostly in postmenopausal women due to a lack of the hormone oestrogen, which helps to regulate the incorporation of calcium into the bones. Osteoporosis tends to occur mostly among postmenopausal women aged between 51 and 75. It can occur earlier, or later
and not all women are at equal risk of developing osteoporosis. Osteoporosis is sometimes called the silent disease as there are often no symptoms until a fracture occurs. Although the whole skeleton is usually affected fractures mostly occur in the wrist, spine and hip. One in two women and one in five men in the UK will suffer a fracture after the age of 50; in fact every three minutes someone has afracture due to osteoporosis However, osteoporosis has been diagnosed in people as young as 20. The dairy industry has responded to this health scare by promoting the consumption of milk, cheese and yogurt directly to teenage girls. However, American women are among the biggest consumers of calcium in the world yet they have one of the highest levels of osteoporosis African Bantu women, on the other hand, eat almost no dairy products at all; they have a relatively low calcium intake, mainly from vegetable sources, and typically have up to 10 children each. Yet osteoporosis is virtually unknown among Bantu women. It seems that the more dairy produce we consume, the higher our risk of fracture. The Harvard Nurses Health study examined whether higher intakes of milk can reduce the risk of osteoporotic fractures. The study observed over 75000 women for 12 years and concluded that increasing milk consumption did not confer a protective effect against hip or forearm fracture. In fact the report suggested that an increased calcium intake from dairy foods was associated with a higher risk of fracture. It has been suggested that calcium loss from the bone is promoted by a high intake of animal protein. One study of 1600 older women examined the level of bone loss and found vegetarians had only 18 per cent less bone mineral compared to omnivores who had lost 35 per cent bone mineral by the age of 80 Another study of 1035 elderly women found that women with a high ratio of animal to vegetable protein intake had a greater risk of hip fracture than those with a low ratio. In a similar study that analysed the incidence of hip fracture in relation to the consumption of animal and vegetable protein in 33 countries it was concluded that moderating the consumption of animal food might protect against hip fracture Cross-cultural studies summarising data on protein intake and fracture rates from 16 countries compared industrialised and non-industrialised lifestyles and revealed strong links between a high animal protein diet, bone degeneration and the occurrence of hip fractures In Professor T. Colin Campbell’s extensive ‘China Study’ (the largest study in the world of the effects of diet on health) Campbell observed that in rural communities where animal protein made up just 10 per cent of the total protein intake (the other 90 per cent coming from plant-based sources) the bone fracture rate was one-fifth of that in the US where a much higher ratio of animal to vegetable protein is consumed again indicating a link between animal protein and bone degeneration.
But what is the mechanism for this process? As food is digested acids are released into the blood, the body attempts to neutralise the acid by drawing calcium from the bones. This calcium is then excreted in the urine (the calciuric response). Animal protein has a particularly bad effect because of the greater amount of sulphur-containing amino acids it contains compared to plant protein. As the sulphur content of the diet increases so does the level of calcium in the urine. Studies reveal that an animal protein diet (with the same total quantity of protein as a vegetarian diet) confers an increased risk for uric acid stones. Furthermore the animal-protein induced calciuric response may be a risk factor for the development of osteoporosis. The traditional Inuit (or Eskimo) diet is made up almost entirely of animal protein. Inuits potentially have one of the highest calcium intakes in the world (up to 2,500 mg a day) depending on whether they eat whole fish, including the bones, or not. They also have a high rate of osteoporosis, even higher than white Americans. There are many factors linked to bone health that may even be more important than calcium. For example, when the bone density of 80 young women was monitored over a 10-year period, it showed that exercise was more important than calcium intake In older people, a 15-year investigation into whether low calcium intake was a risk factor for hip fractures concluded that cutting back on dairy did not increase the risk and that physical activity provided better protection The discovery of 18th-century human bones under a London church revealed that today’s women lose far more calcium than our ancestors This may be
attributed to a lower degree of physical activity. This research supports an increasing amount of evidence that physical activity is a key factor in reducing osteoporosis risk.
To promote bone health and reduce the risk of osteoporosis it is important to get enough vitamin D, reduce caffeine and alcohol intake and not smoke. Many studies suggest exercise is the most important determining factor. The best type of activity for bone health is weight bearing exercise; this includes walking, stair climbing and dancing.
The amount of calcium present in a particular food is not the only important, factor to consider. The bioavailability of the calcium should be considered when deciding which foods are a good source. This means how much calcium is actually available for absorption into the body from the food. The calcium in dairy products is not as well absorbed as that in many dark green leafy vegetables For example, calcium absorbability from kale was demonstrated to be considerably higher than that from cow’s milk While spinach contains a relatively high amount of calcium, it is bound to a substance called oxalate which hinders calcium absorption so it is important to obtain calcium from low-oxalate green vegetables. Grains, nuts and seeds contain a substance called phytic acid which until recently was also considered to hinder calcium absorption, now phytic acid is believed to have only a minor influence Caffeine and smoking have been shown to reduce calcium absorption.
Vitamin D
The body requires vitamin D to absorb and retain calcium in the bones. Vitamin D is either obtained from the diet or it is synthesised in the skin following exposure to sunlight. But recent concerns about skin cancer have encouraged us to cover up and avoid the sun. Subsequently people in the UK could be at risk of vitamin D deficiency if they get too little sun exposure year round Without sufficient vitamin D, calcium deficiency is likely to occur even if the diet provides enough calcium. The consequences may be serious, resulting in rickets or osteomalacia (softening of the bones). Over the last few years there have been cases of vitamin D deficiency in some large UK cities Vegans obtain vitamin D from sunlight and fortified foods such as soya milks, cereals and margarines. It is important to get the balance right between being cautious about exposure to the sun and aware of the need for some exposure. It is now advised by the UK government that we apply sun block after 10 to 15 minutes exposure to the sun, this is so that we can synthesise vitamin D in the skin.
Magnesium, Potassium, Vitamin C and Vitamin K
Magnesium, potassium, vitamin C and vitamin K are all required for good bone health. A healthy diet that includes at least five servings a day of
fruit and vegetables should optimise the intake of these and other micronutrients required.
Animal Protein and Osteoporosis
Bones consist of a thick outer shell and a strong inner mesh filled with a protein called collagen, calcium salts and other minerals. Osteoporosis (meaning porous bones) occurs when calcium is lost from the bones and they become more fragile and prone to fracture. This debilitating condition tends to occur mostly in postmenopausal women due to a lack of the hormone oestrogen, which helps to regulate the incorporation of calcium into the bones. Osteoporosis tends to occur mostly among postmenopausal women aged between 51 and 75. It can occur earlier, or later
and not all women are at equal risk of developing osteoporosis. Osteoporosis is sometimes called the silent disease as there are often no symptoms until a fracture occurs. Although the whole skeleton is usually affected fractures mostly occur in the wrist, spine and hip. One in two women and one in five men in the UK will suffer a fracture after the age of 50; in fact every three minutes someone has afracture due to osteoporosis However, osteoporosis has been diagnosed in people as young as 20. The dairy industry has responded to this health scare by promoting the consumption of milk, cheese and yogurt directly to teenage girls. However, American women are among the biggest consumers of calcium in the world yet they have one of the highest levels of osteoporosis African Bantu women, on the other hand, eat almost no dairy products at all; they have a relatively low calcium intake, mainly from vegetable sources, and typically have up to 10 children each. Yet osteoporosis is virtually unknown among Bantu women. It seems that the more dairy produce we consume, the higher our risk of fracture. The Harvard Nurses Health study examined whether higher intakes of milk can reduce the risk of osteoporotic fractures. The study observed over 75000 women for 12 years and concluded that increasing milk consumption did not confer a protective effect against hip or forearm fracture. In fact the report suggested that an increased calcium intake from dairy foods was associated with a higher risk of fracture. It has been suggested that calcium loss from the bone is promoted by a high intake of animal protein. One study of 1600 older women examined the level of bone loss and found vegetarians had only 18 per cent less bone mineral compared to omnivores who had lost 35 per cent bone mineral by the age of 80 Another study of 1035 elderly women found that women with a high ratio of animal to vegetable protein intake had a greater risk of hip fracture than those with a low ratio. In a similar study that analysed the incidence of hip fracture in relation to the consumption of animal and vegetable protein in 33 countries it was concluded that moderating the consumption of animal food might protect against hip fracture Cross-cultural studies summarising data on protein intake and fracture rates from 16 countries compared industrialised and non-industrialised lifestyles and revealed strong links between a high animal protein diet, bone degeneration and the occurrence of hip fractures In Professor T. Colin Campbell’s extensive ‘China Study’ (the largest study in the world of the effects of diet on health) Campbell observed that in rural communities where animal protein made up just 10 per cent of the total protein intake (the other 90 per cent coming from plant-based sources) the bone fracture rate was one-fifth of that in the US where a much higher ratio of animal to vegetable protein is consumed again indicating a link between animal protein and bone degeneration.
But what is the mechanism for this process? As food is digested acids are released into the blood, the body attempts to neutralise the acid by drawing calcium from the bones. This calcium is then excreted in the urine (the calciuric response). Animal protein has a particularly bad effect because of the greater amount of sulphur-containing amino acids it contains compared to plant protein. As the sulphur content of the diet increases so does the level of calcium in the urine. Studies reveal that an animal protein diet (with the same total quantity of protein as a vegetarian diet) confers an increased risk for uric acid stones. Furthermore the animal-protein induced calciuric response may be a risk factor for the development of osteoporosis. The traditional Inuit (or Eskimo) diet is made up almost entirely of animal protein. Inuits potentially have one of the highest calcium intakes in the world (up to 2,500 mg a day) depending on whether they eat whole fish, including the bones, or not. They also have a high rate of osteoporosis, even higher than white Americans. There are many factors linked to bone health that may even be more important than calcium. For example, when the bone density of 80 young women was monitored over a 10-year period, it showed that exercise was more important than calcium intake In older people, a 15-year investigation into whether low calcium intake was a risk factor for hip fractures concluded that cutting back on dairy did not increase the risk and that physical activity provided better protection The discovery of 18th-century human bones under a London church revealed that today’s women lose far more calcium than our ancestors This may be
attributed to a lower degree of physical activity. This research supports an increasing amount of evidence that physical activity is a key factor in reducing osteoporosis risk.
To promote bone health and reduce the risk of osteoporosis it is important to get enough vitamin D, reduce caffeine and alcohol intake and not smoke. Many studies suggest exercise is the most important determining factor. The best type of activity for bone health is weight bearing exercise; this includes walking, stair climbing and dancing.
|
Summary
• Children and young adults do not need dairy foods for good bone health; they do need exercise and a healthy plant-based diet to ensure strong bones. • Diets loaded with dairy products are associated with an increased risk of many diseases including osteoporosis, cancer, heart disease, obesity and diabetes. • From a health perspective, dairy foods should be avoided in the diet. • Cow’s milk is not a natural food for humans to consume. • Most people in the world cannot digest the sugar in milk - lactose, and are known as lactose intolerant. Therefore, the vast majority of people obtain calcium from plant-based sources.• Many children are affected by cow’s milk allergies. |
• Looking solely at calcium intake and not at calcium losses tells only half the story, while a vegan’s intake might be less than a meat eater’s, their losses are likely to be much lower. A plant based diet free of animal products - a vegan diet – does not produce these losses. • There are no scientific reports of calcium deficiency in adult vegans. • Vitamin D, magnesium, potassium, vitamin C and vitamin K are all required for good bone health. • Plant-based sources of calcium are many and varied and offer many other health benefits as well as providing a natural and safe source of calcium. |
Why public health strategy should promote plant oils in preference to fish oils

Fish is seemingly promoted as the new penicillin. VVF uncovers the science to show that it is plant oils and a plant based diet, not fish oils, that are the real way forward for lifelong health.
Introduction
People are encouraged to believe that a healthy diet is one which includes fish. The reason being that some fish contain the types of ‘good’ fat that our bodies need. There is a widespread misconception amongst the general public and health professionals that fish is the only source of these good fats. There are two reasons why these ideas have become so well established. Firstly, much has been made of the healthiness of the Mediterranean diet, which is based on generous servings of fruits and vegetables, cereals and olive oil and where fish is served in preference to meat or dairy products. Mealtimes tend to be very social and this may have profound implications for health. Secondly, a number of studies have examined the effect of fish in helping to prevent a second heart attack in people who have already had one attack and these show some protection benefits.
Fats in the Diet
There’s a lot of confusion about fat and diet, but the truth is that our bodies can’t function without it. Eating the right kind of fat is, however crucial. What we don’t need are saturated fats, found mainly in meat, dairy and animal products, but also in many processed foods. These are strongly linked to high blood cholesterol, hardening of the arteries, coronary heart disease, some cancers and other degenerative diseases. We do need unsaturated fats - especially polyunsaturated fats. Within polyunsaturated fats are substances called essential fatty acids, or EFAs - namely omega-6 (linoleic acid - LA) and omega-3 fats (linolenic acid - LNA). Although olive oil is not an EFA it is another type of unsaturated fat which has some healthy properties and it is good to include it in the diet. EFAs - particularly the omega-3 fats - help keep the heart healthy. Fish is a source of EFAs, particularly omega-3 fats, but not all fish contain them. Those that do are principally oily fish such as herring, salmon, mackerel, sardines and fresh tuna. White fish, such as cod, haddock and plaice, don’t and nor does tinned tuna. However, the richest sources of omega-3 fats are not fish at all but plants. Seed oils such as linseed (flax) and rapeseed (canola) as well as soya oil are rich sources as are seeds and nuts themselves - particularly walnuts. Green leafy vegetables are also a source.
Omega-3 and Heart Disease
It’s been known for a long time that people whose diet is based largely on fish and is rich in omega-3 have low rates of heart disease. This led researchers to investigate whether giving fish to people who had already suffered a heart attack would prevent them from having another attack. These are ‘secondary prevention trials’ and two of the largest are the DART and GISSI trials, which both used fish-based omega-3 fats. They did show a reduced risk, but much less publicised was the LYON trial, which used plant oils as a source of omega-3 fats. The results of this study showed that plant oils reduced the riskof a secondary heart attack by at least twice that of fish oils!
Introduction
People are encouraged to believe that a healthy diet is one which includes fish. The reason being that some fish contain the types of ‘good’ fat that our bodies need. There is a widespread misconception amongst the general public and health professionals that fish is the only source of these good fats. There are two reasons why these ideas have become so well established. Firstly, much has been made of the healthiness of the Mediterranean diet, which is based on generous servings of fruits and vegetables, cereals and olive oil and where fish is served in preference to meat or dairy products. Mealtimes tend to be very social and this may have profound implications for health. Secondly, a number of studies have examined the effect of fish in helping to prevent a second heart attack in people who have already had one attack and these show some protection benefits.
Fats in the Diet
There’s a lot of confusion about fat and diet, but the truth is that our bodies can’t function without it. Eating the right kind of fat is, however crucial. What we don’t need are saturated fats, found mainly in meat, dairy and animal products, but also in many processed foods. These are strongly linked to high blood cholesterol, hardening of the arteries, coronary heart disease, some cancers and other degenerative diseases. We do need unsaturated fats - especially polyunsaturated fats. Within polyunsaturated fats are substances called essential fatty acids, or EFAs - namely omega-6 (linoleic acid - LA) and omega-3 fats (linolenic acid - LNA). Although olive oil is not an EFA it is another type of unsaturated fat which has some healthy properties and it is good to include it in the diet. EFAs - particularly the omega-3 fats - help keep the heart healthy. Fish is a source of EFAs, particularly omega-3 fats, but not all fish contain them. Those that do are principally oily fish such as herring, salmon, mackerel, sardines and fresh tuna. White fish, such as cod, haddock and plaice, don’t and nor does tinned tuna. However, the richest sources of omega-3 fats are not fish at all but plants. Seed oils such as linseed (flax) and rapeseed (canola) as well as soya oil are rich sources as are seeds and nuts themselves - particularly walnuts. Green leafy vegetables are also a source.
Omega-3 and Heart Disease
It’s been known for a long time that people whose diet is based largely on fish and is rich in omega-3 have low rates of heart disease. This led researchers to investigate whether giving fish to people who had already suffered a heart attack would prevent them from having another attack. These are ‘secondary prevention trials’ and two of the largest are the DART and GISSI trials, which both used fish-based omega-3 fats. They did show a reduced risk, but much less publicised was the LYON trial, which used plant oils as a source of omega-3 fats. The results of this study showed that plant oils reduced the riskof a secondary heart attack by at least twice that of fish oils!
DART Trial

It found that males who had been advised to eat as much as 400g of oily fish per week showed a reduction of almost 30 per cent in mortality (death) over two years. Although there were fewer fatal heart attacks, the total number of heart attacks wasn’t reduced. It is thought that fish oils help to normalise heartbeat rhythms and prevent blood from becoming too sticky and ‘clumping’. Despite this apparent reduction in risk, a follow-up study 10 years later found there were no long-term survival benefits.
GISSI Trial
This trial looked at people on a Mediterranean diet who had had a heart attack and survived it. Fish oil supplements equivalent to a whopping 100g of oily fish per day were given and showed a 20 per cent reduction in mortality.
LYON Trial
This was another secondary prevention trial, but instead of fish or fish oils, plant-derived omega-3 fatty acids were used. Amazingly, a 70 per cent reduction in mortality was achieved - more than double that of the fish trials! There was also a significant reduction in coronary ‘events’ and these protective effects were found to start quickly. Four years on, patients were still following the diet and their hearts were still being protected. Subsequent studies have confirmed the power of plant omega-3 fatty acids in protecting the heart.
Plant Oils Better than Fish Oils
Comparing the three main trials shows that:
• plant oils are far more effective than fish oils in reducing the
chance of cardiac death in high-risk patients;
• plant oils reduce the risk of dying from secondary heart attack
by more than double that of fish oils;
• plant oils reduce the number of painful, non-fatal heart attacks;
• there are long-term survival benefits from consuming plant oils.
No Gain for Low-Risk
The trials we’ve written about all looked at people who were at high risk of a heart attack. Because people are termed ‘low-risk’, it doesn't mean they will never have an attack, it simply means they are further down the risk scale. They are those who eat low levels of saturated fat and therefore can include vegetarians and vegans. When researchers looked at low-risk groups they found that eating fish had no effect on reducing their chances of dying from a heart attack.
Toxins in Fish
Human beings have been so successful at spreading pollution that environmental contamination is widespread and all oceans now contain toxic chemicals. Persistent organic pollutants (POPs) are now part of most food chains and they become more concentrated the higher up the chain you go. Mercury, organophosphates, PCBs, dioxins, and radioactive pollution in some fish, are all highly toxic to life. Fatty foods have a tendency to ‘soak’ up toxins and so oily fish areparticularly prone to absorbing them - the toxins are actually stored in the fatty part of the fish. By eating smaller fish, oily fish take on their toxic load and become ever more toxic themselves! POPs are implicated in heart disease, infertility and can harm developing foetuses. Responding to a Food Standards Agency 2002 survey, the Consumers’ Association warned that high levels of dioxins and PCBs in fish and fish oil supplements could “put millions at risk”
This trial looked at people on a Mediterranean diet who had had a heart attack and survived it. Fish oil supplements equivalent to a whopping 100g of oily fish per day were given and showed a 20 per cent reduction in mortality.
LYON Trial
This was another secondary prevention trial, but instead of fish or fish oils, plant-derived omega-3 fatty acids were used. Amazingly, a 70 per cent reduction in mortality was achieved - more than double that of the fish trials! There was also a significant reduction in coronary ‘events’ and these protective effects were found to start quickly. Four years on, patients were still following the diet and their hearts were still being protected. Subsequent studies have confirmed the power of plant omega-3 fatty acids in protecting the heart.
Plant Oils Better than Fish Oils
Comparing the three main trials shows that:
• plant oils are far more effective than fish oils in reducing the
chance of cardiac death in high-risk patients;
• plant oils reduce the risk of dying from secondary heart attack
by more than double that of fish oils;
• plant oils reduce the number of painful, non-fatal heart attacks;
• there are long-term survival benefits from consuming plant oils.
No Gain for Low-Risk
The trials we’ve written about all looked at people who were at high risk of a heart attack. Because people are termed ‘low-risk’, it doesn't mean they will never have an attack, it simply means they are further down the risk scale. They are those who eat low levels of saturated fat and therefore can include vegetarians and vegans. When researchers looked at low-risk groups they found that eating fish had no effect on reducing their chances of dying from a heart attack.
Toxins in Fish
Human beings have been so successful at spreading pollution that environmental contamination is widespread and all oceans now contain toxic chemicals. Persistent organic pollutants (POPs) are now part of most food chains and they become more concentrated the higher up the chain you go. Mercury, organophosphates, PCBs, dioxins, and radioactive pollution in some fish, are all highly toxic to life. Fatty foods have a tendency to ‘soak’ up toxins and so oily fish areparticularly prone to absorbing them - the toxins are actually stored in the fatty part of the fish. By eating smaller fish, oily fish take on their toxic load and become ever more toxic themselves! POPs are implicated in heart disease, infertility and can harm developing foetuses. Responding to a Food Standards Agency 2002 survey, the Consumers’ Association warned that high levels of dioxins and PCBs in fish and fish oil supplements could “put millions at risk”
Mercury in Fish
Humans should avoid mercury in their diet as it acts like a poison, affecting their kidneys, heart and central nervous system (CNS). Exposure to mercury is a particular risk for unborn children where the main organs, especially the CNS, are still developing. According to a government agency, fish eating is responsible for the majority of mercury in people’s diets. Following a Food Standards Agency survey of mercury levels in fish, official advice is now for pregnant and breastfeeding women to limit how much tuna they eat and for them and children under 16 not to eat shark, swordfish or marlin at all. Other studies have found that over 60 per cent of bluefin tuna caught in the Mediterranean exceed EC ‘safety’ figures. Researchers have calculated that some of those people who eat high levels of these oily fish will far exceed the World HealthOrganisation’s (WHO) ‘safety’ levels A 2000 government study failed to detect any mercury in vegetarian diets and concluded, “it is reasonable to assume that because participants in this study did not eat fish, their dietary exposures to mercury will be substantially less than those of the general population”.
Protect and Survive
One way mercury harms the body is by acting as a potent free radical. Free radicals are unstable molecules that damage body cells and the body’s main defence against them are antioxidants - betacarotene (converted to vitamin A), and vitamins C and E. Plant foods are rich in these antioxidants and plant oils are particularly rich in vitamin E, which stops EFAs from deteriorating or going off. Only plant oils, not fish oils, contain protective vitamin E.
How Much Fish?
The FSA seem as muddled as everyone else about how much fish people should eat each week. Some of its publications say two servings and others say at least two servings. But, in any case, surveys show the vast majority of people are unaware of the official advice and most people are confused by what is meant by oily fish.
Public Health Failure
The average UK consumption of oily fish is 53g per person per week. This meagre quantity represents only about a third of a single portion and is a tiny amount compared to the 400g weekly intake of oily fish which have been used to produce heart benefits in research studies. This shows that all the attempts to get the British public to eat fish is a spectacular failure.
Alternatives to Fish Oils
Seeds, nuts, beans and their oils are the richest-known sources of the ‘good’ fats. Green leafy vegetables also contain these essential fats. Walnuts, linseed (flaxseed) and rapeseed oil (canola) are all exceptionally rich in omega-3 fats. The best way to buy and store nuts, seeds and their oils is in very small quantities and to keep them in the fridge. This helps to ensure that they are as fresh as possible. These oils are not suitable for heating as it destroys the beneficial EFAs. Most health food shops and supermarkets sell packets of nuts and seeds and blended plant oils - usually marketed as oils rich in omega-3 and omega-6 fats. They contain information on how much oil to use each day. With whole seeds and nuts, a handful each day is normally sufficient. Olive oil can be used for cooking.
Fishless Foods
Fish-like substitutes are available thanks to food technologists who have produced imitation fish fingers, scampi, tuna and salmon paté that actually taste of fish. They are available in most health food shops.
Intelligent Public Health Promotion
Adding fish to the diet will not bring about long-term good health. Plant-based vegetarian and vegan diets are the best choice for optimum health.
Summary
• Plant oils are a far healthier source of the essential fats we need.
• Plant oils halve the risk of heart disease compared with fish oils.
• Fish is a spectacularly unpopular food in the UK.
• Fish is likely to be contaminated with harmful chemicals.
• Plant oils are far less likely to turn rancid than fish oils.
• Plant oils as nuts and seeds are the ultimate fast food.
• Plant-based diets offer protection against many diseases.
Our hearts don’t need fish, our brains don’t need fish and our health is far better served by plant oils and a well-balanced plant-based diet.
Humans should avoid mercury in their diet as it acts like a poison, affecting their kidneys, heart and central nervous system (CNS). Exposure to mercury is a particular risk for unborn children where the main organs, especially the CNS, are still developing. According to a government agency, fish eating is responsible for the majority of mercury in people’s diets. Following a Food Standards Agency survey of mercury levels in fish, official advice is now for pregnant and breastfeeding women to limit how much tuna they eat and for them and children under 16 not to eat shark, swordfish or marlin at all. Other studies have found that over 60 per cent of bluefin tuna caught in the Mediterranean exceed EC ‘safety’ figures. Researchers have calculated that some of those people who eat high levels of these oily fish will far exceed the World HealthOrganisation’s (WHO) ‘safety’ levels A 2000 government study failed to detect any mercury in vegetarian diets and concluded, “it is reasonable to assume that because participants in this study did not eat fish, their dietary exposures to mercury will be substantially less than those of the general population”.
Protect and Survive
One way mercury harms the body is by acting as a potent free radical. Free radicals are unstable molecules that damage body cells and the body’s main defence against them are antioxidants - betacarotene (converted to vitamin A), and vitamins C and E. Plant foods are rich in these antioxidants and plant oils are particularly rich in vitamin E, which stops EFAs from deteriorating or going off. Only plant oils, not fish oils, contain protective vitamin E.
How Much Fish?
The FSA seem as muddled as everyone else about how much fish people should eat each week. Some of its publications say two servings and others say at least two servings. But, in any case, surveys show the vast majority of people are unaware of the official advice and most people are confused by what is meant by oily fish.
Public Health Failure
The average UK consumption of oily fish is 53g per person per week. This meagre quantity represents only about a third of a single portion and is a tiny amount compared to the 400g weekly intake of oily fish which have been used to produce heart benefits in research studies. This shows that all the attempts to get the British public to eat fish is a spectacular failure.
Alternatives to Fish Oils
Seeds, nuts, beans and their oils are the richest-known sources of the ‘good’ fats. Green leafy vegetables also contain these essential fats. Walnuts, linseed (flaxseed) and rapeseed oil (canola) are all exceptionally rich in omega-3 fats. The best way to buy and store nuts, seeds and their oils is in very small quantities and to keep them in the fridge. This helps to ensure that they are as fresh as possible. These oils are not suitable for heating as it destroys the beneficial EFAs. Most health food shops and supermarkets sell packets of nuts and seeds and blended plant oils - usually marketed as oils rich in omega-3 and omega-6 fats. They contain information on how much oil to use each day. With whole seeds and nuts, a handful each day is normally sufficient. Olive oil can be used for cooking.
Fishless Foods
Fish-like substitutes are available thanks to food technologists who have produced imitation fish fingers, scampi, tuna and salmon paté that actually taste of fish. They are available in most health food shops.
Intelligent Public Health Promotion
Adding fish to the diet will not bring about long-term good health. Plant-based vegetarian and vegan diets are the best choice for optimum health.
Summary
• Plant oils are a far healthier source of the essential fats we need.
• Plant oils halve the risk of heart disease compared with fish oils.
• Fish is a spectacularly unpopular food in the UK.
• Fish is likely to be contaminated with harmful chemicals.
• Plant oils are far less likely to turn rancid than fish oils.
• Plant oils as nuts and seeds are the ultimate fast food.
• Plant-based diets offer protection against many diseases.
Our hearts don’t need fish, our brains don’t need fish and our health is far better served by plant oils and a well-balanced plant-based diet.